Hypercholesterolemia: Symptoms, Causes, and Treatment
Hypercholesterolemia represents a public health problem due to its high prevalence. Not only does it go undetected for a long time, but it can also have very detrimental effects in the long run.
If you’re interested in knowing a little more about this condition, we’ve prepared the following article to clarify your doubts. Keep reading!
What is hypercholesterolemia?
Hypercholesterolemia is a condition in which there’s excess cholesterol in the blood. Depending on the cause, it may or may not have a genetic origin.
Although it can remain for a relatively long period of time without producing symptoms, this leads to a higher incidence of fatal cardiovascular events in the future. The medical community has studied it in order to understand the scope as a risk factor.
What is cholesterol?
Cholesterol is a type of lipid (fat) with a large and complex molecular structure. It can be synthesized in the human body, but it’s common to consume it through the diet. It’s considered vital for the body because it fulfills numerous functions, such as the following:
- It’s part of all cell membranes.
- Steroid hormones such as cortisol and testosterone are synthesized from it.
- It participates in the metabolism of vitamin D, necessary for the intestinal absorption of calcium.
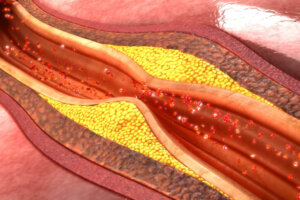
In general, it has a negative connotation, but this is related to the accumulation in the arteries of particles known as LDL (bad cholesterol), which we’ll talk about in the next section. The truth is that the problem is present in the oxidation of these substances rather than in their presence as such.

What are lipoproteins?
One of the most important characteristics of lipids is that, due to their chemical structure, they’re insoluble in water. Therefore, they can’t travel free in the blood either. To be transported from one tissue to another, they need to bind to proteins, which can be soluble. This gives rise to lipoproteins, which are molecular complexes linked to atherosclerosis.
How many types are there?
The most important lipoproteins are the following:
- LDL (low density lipoprotein): This is formed in the liver and, from there, it’s distributed to the rest of the tissues. Due to its ability to be stored in the walls of blood vessels, it’s known as bad cholesterol, as it promotes cardiovascular disease (CVD).
- HDL (high-density lipoproteins): Contrary to LDL, this molecule is responsible for returning cholesterol from the different tissues to the liver when there’s an excess. For this reason it’s called “good” cholesterol, as it prevents the progression of atheromatous plaques.
In addition, cholesterol and lipid metabolism include other important lipoproteins:
- Chylomicron: This is the first large molecule that’s formed after the absorption of lipids in the digestive system. It can travel through the lymphatic system and then enter the venous system, from where it travels to the liver and other tissues.
- VLDL (Very Low Density Lipoprotein): Contains triglycerides and also originates in the liver.
The symptoms of hypercholesterolemia
It’s very difficult to determine that someone has high cholesterol from symptoms alone. This is due to the fact that, like arterial hypertension, it’s a silent disease that doesn’t usually produce manifestations until it’s too late.
In fact, many patients with hypercholesterolemia find out that they had this condition when they suffer a cardiovascular event. These include, for example, episodes of angina pectoris, myocardial infarctions, and peripheral arterial disease.
In familial hypercholesterolemia, things can change a bit. This condition is a variation that’s related to genetic defects in lipid metabolism. It is called familial because it’s inherited.
In the most serious cases, patients don’t have a good life expectancy and usually die from complications. In addition, they can manifest obvious external symptoms. These are produced by the deposit of cholesterol in different tissues:
- Xanthelasmas: They’re visualized as bumps around the eyelids and eyes.
- Xanthomas: They’re the same as the previous case, but in the tendons and joints.
- Corneal arch: This is a faint ring color that’s observed in the periphery of the iris. It closely resembles the senile arc that appears in elderly patients.
How do you make a diagnosis?
This only requires a simple blood test. What’s determined is the amount of cholesterol and triglycerides, in addition to the levels of LDL, HDL, and VLDL.
Based on the limits established by the manufacturer of the reagents and each laboratory, the study can estimate if the patient suffers from hypercholesterolemia. Other conditions, such as hypertriglyceridemia, can also be detected.
Main causes of hypercholesterolemia
This condition is multicausal, although in general terms it occurs for two reasons:
- Genetic defects present at birth.
- Environmental factors likely to be modified.
1. Genetic alterations (familial hypercholesterolemia)
It is a serious disorder whose development depends on the genes inherited from each parent. The fundamental defect is in the production of LDL receptors.
The receptors are proteins responsible for introducing LDL from the blood into the cells of any tissue. LDL particles accumulate and form atheromatous plaques.
Fortunately, most cases produce moderate elevations in cholesterol. A low percentage of patients develop the complete and more severe form of the disease. They tend to die at a very early age from cardiovascular complications.
2. Bad dietary habits
Of course, a diet high in processed carbohydrates and excess lipids can lead to the development of hypercholesterolemia. In fact, it is known that about 50% of blood cholesterol is provided through food intake.
A diet rich in fruits and vegetables and with constant physical activity helps prevent the development of hypercholesterolemia. These foods contain micronutrients, antioxidants, and other chemical compounds that not only regulate lipid metabolism, but also help prevent certain chronic diseases.
3. Smoking
Chronic cigarette smoking affects numerous bodily functions. In fact, nicotine has the ability to induce lipid synthesis. This increases the amount of LDL in the blood and decreases the amount of HDL.
Another of the effects of smoking includes damage to the wall of the arteries, with the consequent elevation of blood pressure. High blood pressure is also linked to growth and permanent damage to the heart. This can lead to the development of a very important clinical syndrome known as heart failure.

Risk factors that increase mortality
Patients with hypercholesterolemia often have associated chronic conditions that worsen the prognosis. Some of them are the following:
- Arterial hypertension: a chronic and silent disease that can cause permanent damage to the heart.
- Obesity: is a condition that has the ability to alter blood lipids.
- Sedentary lifestyle: the absence of physical exercise favors the appearance of obesity.
- Diabetes mellitus: one of the best-known metabolic diseases that, due to poor insulin management, can also lead to dyslipidemia.
Is there treatment for hypercholesterolemia?
The management of these pathologies includes lifestyle changes and drugs. Lifestyle changes mean eating a healthy diet and sustaining physical exercise. At first, this is usually low impact to allow the body to adapt to this modification.
The drugs used are very varied and each one acts in different places:
- Statins: a classic example is atorvastatin and they are responsible for reducing the endogenous synthesis of cholesterol.
- Resins: These are ingested and bind to cholesterol-containing bile acids, preventing their absorption. A representative example is cholestyramine.
- Fibrates – Affect lipid metabolism and are used in various medical conditions, such as diabetes and hypothyroidism.
- Nicotinic acid: it is a derivative of vitamin B that inhibits the synthesis of some compounds necessary for the creation of LDL.
A medical professional will be in charge of determining the need to use one or the other drug. Doses vary according to the severity of cholesterol levels, as do monodrug combinations.
Hypercholesterolemia represents a public health problem due to its high prevalence. Not only does it go undetected for a long time, but it can also have very detrimental effects in the long run.
If you’re interested in knowing a little more about this condition, we’ve prepared the following article to clarify your doubts. Keep reading!
What is hypercholesterolemia?
Hypercholesterolemia is a condition in which there’s excess cholesterol in the blood. Depending on the cause, it may or may not have a genetic origin.
Although it can remain for a relatively long period of time without producing symptoms, this leads to a higher incidence of fatal cardiovascular events in the future. The medical community has studied it in order to understand the scope as a risk factor.
What is cholesterol?
Cholesterol is a type of lipid (fat) with a large and complex molecular structure. It can be synthesized in the human body, but it’s common to consume it through the diet. It’s considered vital for the body because it fulfills numerous functions, such as the following:
- It’s part of all cell membranes.
- Steroid hormones such as cortisol and testosterone are synthesized from it.
- It participates in the metabolism of vitamin D, necessary for the intestinal absorption of calcium.
In general, it has a negative connotation, but this is related to the accumulation in the arteries of particles known as LDL (bad cholesterol), which we’ll talk about in the next section. The truth is that the problem is present in the oxidation of these substances rather than in their presence as such.
What are lipoproteins?
One of the most important characteristics of lipids is that, due to their chemical structure, they’re insoluble in water. Therefore, they can’t travel free in the blood either. To be transported from one tissue to another, they need to bind to proteins, which can be soluble. This gives rise to lipoproteins, which are molecular complexes linked to atherosclerosis.
How many types are there?
The most important lipoproteins are the following:
- LDL (low density lipoprotein): This is formed in the liver and, from there, it’s distributed to the rest of the tissues. Due to its ability to be stored in the walls of blood vessels, it’s known as bad cholesterol, as it promotes cardiovascular disease (CVD).
- HDL (high-density lipoproteins): Contrary to LDL, this molecule is responsible for returning cholesterol from the different tissues to the liver when there’s an excess. For this reason it’s called “good” cholesterol, as it prevents the progression of atheromatous plaques.
In addition, cholesterol and lipid metabolism include other important lipoproteins:
- Chylomicron: This is the first large molecule that’s formed after the absorption of lipids in the digestive system. It can travel through the lymphatic system and then enter the venous system, from where it travels to the liver and other tissues.
- VLDL (Very Low Density Lipoprotein): Contains triglycerides and also originates in the liver.
The symptoms of hypercholesterolemia
It’s very difficult to determine that someone has high cholesterol from symptoms alone. This is due to the fact that, like arterial hypertension, it’s a silent disease that doesn’t usually produce manifestations until it’s too late.
In fact, many patients with hypercholesterolemia find out that they had this condition when they suffer a cardiovascular event. These include, for example, episodes of angina pectoris, myocardial infarctions, and peripheral arterial disease.
In familial hypercholesterolemia, things can change a bit. This condition is a variation that’s related to genetic defects in lipid metabolism. It is called familial because it’s inherited.
In the most serious cases, patients don’t have a good life expectancy and usually die from complications. In addition, they can manifest obvious external symptoms. These are produced by the deposit of cholesterol in different tissues:
- Xanthelasmas: They’re visualized as bumps around the eyelids and eyes.
- Xanthomas: They’re the same as the previous case, but in the tendons and joints.
- Corneal arch: This is a faint ring color that’s observed in the periphery of the iris. It closely resembles the senile arc that appears in elderly patients.
How do you make a diagnosis?
This only requires a simple blood test. What’s determined is the amount of cholesterol and triglycerides, in addition to the levels of LDL, HDL, and VLDL.
Based on the limits established by the manufacturer of the reagents and each laboratory, the study can estimate if the patient suffers from hypercholesterolemia. Other conditions, such as hypertriglyceridemia, can also be detected.
Main causes of hypercholesterolemia
This condition is multicausal, although in general terms it occurs for two reasons:
- Genetic defects present at birth.
- Environmental factors likely to be modified.
1. Genetic alterations (familial hypercholesterolemia)
It is a serious disorder whose development depends on the genes inherited from each parent. The fundamental defect is in the production of LDL receptors.
The receptors are proteins responsible for introducing LDL from the blood into the cells of any tissue. LDL particles accumulate and form atheromatous plaques.
Fortunately, most cases produce moderate elevations in cholesterol. A low percentage of patients develop the complete and more severe form of the disease. They tend to die at a very early age from cardiovascular complications.
2. Bad dietary habits
Of course, a diet high in processed carbohydrates and excess lipids can lead to the development of hypercholesterolemia. In fact, it is known that about 50% of blood cholesterol is provided through food intake.
A diet rich in fruits and vegetables and with constant physical activity helps prevent the development of hypercholesterolemia. These foods contain micronutrients, antioxidants, and other chemical compounds that not only regulate lipid metabolism, but also help prevent certain chronic diseases.
3. Smoking
Chronic cigarette smoking affects numerous bodily functions. In fact, nicotine has the ability to induce lipid synthesis. This increases the amount of LDL in the blood and decreases the amount of HDL.
Another of the effects of smoking includes damage to the wall of the arteries, with the consequent elevation of blood pressure. High blood pressure is also linked to growth and permanent damage to the heart. This can lead to the development of a very important clinical syndrome known as heart failure.
Risk factors that increase mortality
Patients with hypercholesterolemia often have associated chronic conditions that worsen the prognosis. Some of them are the following:
- Arterial hypertension: a chronic and silent disease that can cause permanent damage to the heart.
- Obesity: is a condition that has the ability to alter blood lipids.
- Sedentary lifestyle: the absence of physical exercise favors the appearance of obesity.
- Diabetes mellitus: one of the best-known metabolic diseases that, due to poor insulin management, can also lead to dyslipidemia.
Is there treatment for hypercholesterolemia?
The management of these pathologies includes lifestyle changes and drugs. Lifestyle changes mean eating a healthy diet and sustaining physical exercise. At first, this is usually low impact to allow the body to adapt to this modification.
The drugs used are very varied and each one acts in different places:
- Statins: a classic example is atorvastatin and they are responsible for reducing the endogenous synthesis of cholesterol.
- Resins: These are ingested and bind to cholesterol-containing bile acids, preventing their absorption. A representative example is cholestyramine.
- Fibrates – Affect lipid metabolism and are used in various medical conditions, such as diabetes and hypothyroidism.
- Nicotinic acid: it is a derivative of vitamin B that inhibits the synthesis of some compounds necessary for the creation of LDL.
A medical professional will be in charge of determining the need to use one or the other drug. Doses vary according to the severity of cholesterol levels, as do monodrug combinations.
- Berrade S, Oyarzábal M, Chueca M. Genética de la hipercolesterolemia familiar.
Indicaciones de los estudios genéticos y su utilidad. Rev Esp Endocrinol Pediatr 2012;3:75-80. - Martínez-Ortiz, J. A., L. Páez, and K. von Saalfeld. “Tratamiento de dislipidemias con ácido nicotínico.” Revista Costarricense de Cardiología 4.1 (2002): 23-27.
- Carretero M. Hipercolesterolemia, diagnóstico y tratamiento. Elsevier 2008;27(9):109-111.
- Riesco J, Serranilla M. Tabaco y lípidos: una asociación que incrementa el riesgo de enfermedad cardiovascular. Patología Respiratoria 2010;13(3):112-113.
- Espondaburu, Omar Raúl. “Hipertrigliceridemia: influencia sobre parámetros que estiman el transporte reverso del colesterol.” Acta bioquímica clínica latinoamericana 40.2 (2006): 165-172.
- Mata, Pedro, et al. “Diagnóstico y tratamiento de la hipercolesterolemia familiar en España: documento de consenso.” SEMERGEN-Medicina de Familia 41.1 (2015): 24-33.
- Rosas A, Lama G, Llanos-Zavalaga F, Dunstan J. Prevalencia de obesidad e hipercolesterolemia en trabajadores de una institución estatal de Lima – Perú. Rev Perú Med Exp Salud Pública 2002;19(2):87-92.
- Castillo Arocha, Ivette, et al. “Riesgo cardiovascular según tablas de la OMS, el estudio Framingham y la razón apolipoproteína B/apolipoproteína A1.” Revista Cubana de Investigaciones Biomédicas 29.4 (2010): 479-488.
- Carrascosa, Carlos Fluixá, Antonio Maiques Galán, and M. Franch Taix. “Estatinas: eficacia, seguridad e indicaciones.” Información terapéutica del sistema nacional de salud 28.4 (2004): 89-100.
Este texto se ofrece únicamente con propósitos informativos y no reemplaza la consulta con un profesional. Ante dudas, consulta a tu especialista.







