What Is Smear Microscopy?
Smear microscopy is a laboratory procedure that seeks to detect the presence of bacilli (cylindrical bacteria) through direct observation using an optical microscope. You can use a sputum sample, bodily fluids, or it can also be found in body tissues.
One of those mentioned is the Koch bacillus, also called Mycobacterium tuberculosis ( M. tuberculosis), which transmits tuberculosis (TB).
Overview of tuberculosis
To understand a little better the fundamentals and effectiveness of smear microscopy, we should devote a few lines to the disease that experts seek to diagnose, tuberculosis.
Transmission
Tuberculosis is an infectious disease, transmitted almost exclusively by air. The bacilli are found in the small droplets of saliva that are coughed up by a person infected with pulmonary TB.
The risk of contracting the disease increases when the number of cases increases in a community or when living with the patient for a long time, mainly in poorly ventilated environments.
Although TB can manifest in any organ other than the lungs (extrapulmonary TB), the most common and infectious form is lung disease.
Because the bacillus is oxygen-dependent, patients with pulmonary TB can develop cavities in the lung apices. Here there’s a higher concentration of oxygen and, because of this, a large number of these bacilli lodge there. When coughing, these are expelled through the upper airways in the form of sputum.
The most infectious patients are those with positive smear microscopy, especially if their disease is severe and with cavitation.
Symptoms

The most characteristic symptom of pulmonary TB is a cough with expectoration lasting two or more weeks. These patients are called respiratory symptomatic (RS). They may also have weight loss, night sweats, and chest pain.
Most people who breathe in TB bacilli become infected, but the immune system is able to stop them from multiplying, and inactivates them. In these cases, we’re talking about latent tuberculosis (LTBI).
These people have a small number of live TB bacilli, but they are inactive, have no symptoms, don’t feel sick, have normal chest X-ray results, can’t transmit the disease, and generally have a positive tuberculin test (PPD). In certain situations, TB can become reactivated if they don’t receive treatment for LTBI.
Diagnosis
The true diagnosis of TB can be made by the following methods:
- Bacilloscopy: This is a simple, inexpensive, efficient, and fast procedure to detect suspected TB cases and to follow up on them after treatment. It continues to be the first diagnostic test in many countries where the use of rapid molecular tests is difficult.
- Culture in liquid medium: A culture is the most sensitive bacteriological diagnostic method, and is the gold standard for the detection of TB and the only valid method to follow the patient’s evolution and confirm their cure. Its main disadvantage is the waiting time to obtain the results.
- It’s the best diagnostic method for extrapulmonary TB.
- Until now, Lowenstein-Jensen and Ogawa-Kudoh culture media have been used because they’re simple and less expensive. Using this last technique, it’s possible to increase the number of newly diagnosed patients (up to 30% more) of positive samples than with smear microscopy.
- Cultivation allows the following:
- Confirm the presence of viable bacilli in smear-positive patients.
- Identify the paucibacillary patient (a patient with a low number of bacilli, such as children), which is why its culture is essential in these cases.
- Rule out resistance to treatment and suspicion of nontuberculous mycobacteria.
- Rapid molecular test (Xpert MTB / RIF assay, Xpert MTB / ultra RIF or TB-LAMP): these have been recommended for rapid identification in cerebrospinal fluid samples and biopsies as they are more sensitive tests. They detect DNA from live bacilli, but also non-viable ones.
Smear microscopy: one of the most used diagnostic methods
Being an inexpensive, easy-to-perform, and effective technique, smear microscopy is one of the most popular in certain countries, forming part of strategic public health plans to control the disease.
Utility
- Smear microscopy allows the diagnosis of active TB and helps to know the efficacy of TB treatment in patients.
- It allows us to identify tuberculosis but isn’t specific to this disease, as it also allows us to recognize other acid-fast bacilli (ARB) that belong to the genus Mycobacterium.
What samples can be used for smear microscopy?
As mentioned above, the most frequent sample is that of pulmonary secretion (sputum), but, as it can affect any organ of the body, the doctor can take samples of pleural fluid, cerebrospinal fluid, ascitic fluid, blood, urine, purulent secretion of some abscess, biopsies, etc.
All extrapulmonary organ samples should be processed for culture and, where possible, for rapid molecular testing.
How are smear samples taken?
To collect the sputum sample, a person will spit saliva into a sterile container, usually offered by the laboratory.
- The person must take a deep breath and then cough forcefully several times, in order to expel or cough up the secretion that comes from the lungs and bronchi. The same procedure must be carried out twice more.
- In the case of children or psychiatric patients, specialized personnel can induce the excretion of sputum through procedures that facilitate the drainage or aspiration of secretions.
A suitable expectoration for analysis is recognized as one that is thick and whitish or yellow-green, sometimes bloody.
The container to be used must be wide-mouthed, with a capacity of 40-50 milliliters, a hermetic screw-type closure, made of transparent plastic material resistant to ruptures. It shouldn’t be reused, in order to prevent contamination.
Diagnostic smear microscopy
It’s recommended to take two or three sputum samples. The first sample detects approximately 80% of positive cases (it must be taken during the first medical consultation), the second 15% (it must be taken by the patient upon waking in the morning) and the third, 5%. Samples can also be taken by bronchial lavage or during fiberoptic bronchoscopy.
Bacilloscopy to control the effectiveness of the treatment
Standard TB treatment comprises two phases:
- Intensive phase: lasting an average of 2 months
- Consolidation phase: lasting an average of 6 months
Using smear microscopy, other tests would be requested after 2, 5, and 6 months of treatment. There should be a progressive decrease in positivity, until the smear microscopy becomes negative. In the case of persistent positivity, cultures with a sensitivity test will be performed to determine whether there’s resistance to the treatment and to establish whether what is observed under the microscope are live or dead bacilli.
Preservation of the sample
If the sputum sample is to be collected for smear microscopy, it should be kept in the refrigerator, wrapped, and tightly tied in a plastic bag or at least in a cool place protected from light. It must be taken to the laboratory as soon as possible.
The technique used to perform the smear microscopy
- The most purulent particles in the sample are selected to increase the probability of obtaining the bacilli, and then they are spread with the applicator in the center of the slide, with an even thickness.
- Let it dry.
- Afterwards, it’s passed through a flame 3-4 times without overheating.
- Finally, the Ziehl-Nielsen stain (auramine-rhodamine or resistance stain) is carried out. First, carbolic fuchsin or auramine is applied, then heat is applied and then a mixture of acid and alcohol is added, which act as bleaches, using methylene blue as a contrast dye.
Technique basis
The technique is based on the so-called acid-alcohol resistance. Mycobacteria contain a high content of lipids, including mycolic acids in the cell wall, which allow them to fix the carbolic fuchsin or auramine in their cell wall and to continue to retain it, even after the application of a mixture of acid and alcohol.
By staining the sample with basic fuchsin, the bacteria take on a reddish coloration, and by adding the acidic alcohol, the lipids of the bacteria resist the discoloration. This is why they are called acid-fast bacilli (ARB).
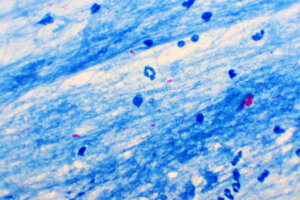
When looking at the slide under a microscope, small fuchsia-red rods are observed on a bluish background. Depending on the staining used, if smears are made with auramine-O staining, these yellow-green fluorescent rods will be observed on a dark background.
BAAR count

The smear is systematically traversed, observing each field of the microscope on the surface and in depth with 10x and 100x lenses (with immersion oil) and the number of BAARs observed in each field are noted. Then, an average of bacilli present is obtained.
It takes approximately 5 minutes to read 100 fields.
How is smear microscopy reported?
At an international level, the following report has been adopted using the Ziehl-Neelsen technique:
- When BAAR is not observed in 100 microscopic fields, it is reported as such: “acid-fast bacilli are not observed.“
- 1 to 9 BAAR in 100 fields: the total number of BAAR found in 100 fields is reported.
- 10 to 99 BAAR in 100 fields: positive (+) is reported.
- 1 to 10 BAAR in 50 fields: positive (++) is reported.
- More than 10 BAAR in 20 fields: positive (+++) is reported.
So if the smear test is positive (+, ++, +++) it means that the patient has TB.
If the smear microscopy reports less than 5 AFB in 100 fields, it’s recommended to extend the reading to 200 fields, perform a PCR test, and use a culture in liquid medium.
The reading and reporting of results of fluorescence-stained sheets has also been established internationally.
If possible, the results should be returned to the health center, within 24 hours of the laboratory receiving the samples.
Quality of smears
To ensure the quality of smears, each laboratory should ensure they do the following:
- Follow the stipulated rules for the proper use of the material, and thus avoid contamination.
- Have proper management of laboratory residues and wastes.
- Internal quality assessment (monitoring of performance indicators).
- External quality assessment (efficiency tests).
How to make smear microscopy a good control tool?
- This is achieved through adequate technical quality and maintaining adequate quality of laboratory records and reports.
- All laboratory services must be integrated into a National Network of Tuberculosis Laboratories and involve public and private laboratories in order to complement each other between the services.
- Procedures must be standardized (periodically reviewed by the Pan American Health Organization (PAHO), World Health Organization (WHO), and the International Union Against Tuberculosis and Respiratory Diseases (LA UNION).
Sensitivity and specificity of smear microscopy
Smear microscopy has a low sensitivity (40-60%) and a very high specificity. Smear microscopy has even lower sensitivity in cases of extrapulmonary disease, children, and patients with HIV / AIDS.
Smear microscopy, present and future
Ziehl-Nielsen staining (smear microscopy) has been the most widely-used technique for the past 100 years, as it requires simpler training.
In TB-endemic countries, a positive smear microscopy of a respiratory sample in an immunocompetent patient has a high predictive value. In other words, the risk of making a mistake when diagnosing the disease is very low.
The laboratory workers who process the samples must always observe the recommended biosafety measures and systematize the activities in order to reduce the risk of contagion.
The risk of contracting tuberculosis increases with the increase in the number of cases in a community, so early diagnosis is essential, with smear microscopy (BK) being a fundamental tool.
New emerging techniques are mercury lamp fluorescence microscopy and, for 10 years, the WHO has recommended the use of LED lamp fluorescence microscopy.
The latter is more sensitive, a totally dark room isn’t needed to read the smears, the reading time is reduced by almost half, and there’s less risk of contamination. However, staff need adequate training.
Smear microscopy is a laboratory procedure that seeks to detect the presence of bacilli (cylindrical bacteria) through direct observation using an optical microscope. You can use a sputum sample, bodily fluids, or it can also be found in body tissues.
One of those mentioned is the Koch bacillus, also called Mycobacterium tuberculosis ( M. tuberculosis), which transmits tuberculosis (TB).
Overview of tuberculosis
To understand a little better the fundamentals and effectiveness of smear microscopy, we should devote a few lines to the disease that experts seek to diagnose, tuberculosis.
Transmission
Tuberculosis is an infectious disease, transmitted almost exclusively by air. The bacilli are found in the small droplets of saliva that are coughed up by a person infected with pulmonary TB.
The risk of contracting the disease increases when the number of cases increases in a community or when living with the patient for a long time, mainly in poorly ventilated environments.
Although TB can manifest in any organ other than the lungs (extrapulmonary TB), the most common and infectious form is lung disease.
Because the bacillus is oxygen-dependent, patients with pulmonary TB can develop cavities in the lung apices. Here there’s a higher concentration of oxygen and, because of this, a large number of these bacilli lodge there. When coughing, these are expelled through the upper airways in the form of sputum.
The most infectious patients are those with positive smear microscopy, especially if their disease is severe and with cavitation.
Symptoms
The most characteristic symptom of pulmonary TB is a cough with expectoration lasting two or more weeks. These patients are called respiratory symptomatic (RS). They may also have weight loss, night sweats, and chest pain.
Most people who breathe in TB bacilli become infected, but the immune system is able to stop them from multiplying, and inactivates them. In these cases, we’re talking about latent tuberculosis (LTBI).
These people have a small number of live TB bacilli, but they are inactive, have no symptoms, don’t feel sick, have normal chest X-ray results, can’t transmit the disease, and generally have a positive tuberculin test (PPD). In certain situations, TB can become reactivated if they don’t receive treatment for LTBI.
Diagnosis
The true diagnosis of TB can be made by the following methods:
- Bacilloscopy: This is a simple, inexpensive, efficient, and fast procedure to detect suspected TB cases and to follow up on them after treatment. It continues to be the first diagnostic test in many countries where the use of rapid molecular tests is difficult.
- Culture in liquid medium: A culture is the most sensitive bacteriological diagnostic method, and is the gold standard for the detection of TB and the only valid method to follow the patient’s evolution and confirm their cure. Its main disadvantage is the waiting time to obtain the results.
- It’s the best diagnostic method for extrapulmonary TB.
- Until now, Lowenstein-Jensen and Ogawa-Kudoh culture media have been used because they’re simple and less expensive. Using this last technique, it’s possible to increase the number of newly diagnosed patients (up to 30% more) of positive samples than with smear microscopy.
- Cultivation allows the following:
- Confirm the presence of viable bacilli in smear-positive patients.
- Identify the paucibacillary patient (a patient with a low number of bacilli, such as children), which is why its culture is essential in these cases.
- Rule out resistance to treatment and suspicion of nontuberculous mycobacteria.
- Rapid molecular test (Xpert MTB / RIF assay, Xpert MTB / ultra RIF or TB-LAMP): these have been recommended for rapid identification in cerebrospinal fluid samples and biopsies as they are more sensitive tests. They detect DNA from live bacilli, but also non-viable ones.
Smear microscopy: one of the most used diagnostic methods
Being an inexpensive, easy-to-perform, and effective technique, smear microscopy is one of the most popular in certain countries, forming part of strategic public health plans to control the disease.
Utility
- Smear microscopy allows the diagnosis of active TB and helps to know the efficacy of TB treatment in patients.
- It allows us to identify tuberculosis but isn’t specific to this disease, as it also allows us to recognize other acid-fast bacilli (ARB) that belong to the genus Mycobacterium.
What samples can be used for smear microscopy?
As mentioned above, the most frequent sample is that of pulmonary secretion (sputum), but, as it can affect any organ of the body, the doctor can take samples of pleural fluid, cerebrospinal fluid, ascitic fluid, blood, urine, purulent secretion of some abscess, biopsies, etc.
All extrapulmonary organ samples should be processed for culture and, where possible, for rapid molecular testing.
How are smear samples taken?
To collect the sputum sample, a person will spit saliva into a sterile container, usually offered by the laboratory.
- The person must take a deep breath and then cough forcefully several times, in order to expel or cough up the secretion that comes from the lungs and bronchi. The same procedure must be carried out twice more.
- In the case of children or psychiatric patients, specialized personnel can induce the excretion of sputum through procedures that facilitate the drainage or aspiration of secretions.
A suitable expectoration for analysis is recognized as one that is thick and whitish or yellow-green, sometimes bloody.
The container to be used must be wide-mouthed, with a capacity of 40-50 milliliters, a hermetic screw-type closure, made of transparent plastic material resistant to ruptures. It shouldn’t be reused, in order to prevent contamination.
Diagnostic smear microscopy
It’s recommended to take two or three sputum samples. The first sample detects approximately 80% of positive cases (it must be taken during the first medical consultation), the second 15% (it must be taken by the patient upon waking in the morning) and the third, 5%. Samples can also be taken by bronchial lavage or during fiberoptic bronchoscopy.
Bacilloscopy to control the effectiveness of the treatment
Standard TB treatment comprises two phases:
- Intensive phase: lasting an average of 2 months
- Consolidation phase: lasting an average of 6 months
Using smear microscopy, other tests would be requested after 2, 5, and 6 months of treatment. There should be a progressive decrease in positivity, until the smear microscopy becomes negative. In the case of persistent positivity, cultures with a sensitivity test will be performed to determine whether there’s resistance to the treatment and to establish whether what is observed under the microscope are live or dead bacilli.
Preservation of the sample
If the sputum sample is to be collected for smear microscopy, it should be kept in the refrigerator, wrapped, and tightly tied in a plastic bag or at least in a cool place protected from light. It must be taken to the laboratory as soon as possible.
The technique used to perform the smear microscopy
- The most purulent particles in the sample are selected to increase the probability of obtaining the bacilli, and then they are spread with the applicator in the center of the slide, with an even thickness.
- Let it dry.
- Afterwards, it’s passed through a flame 3-4 times without overheating.
- Finally, the Ziehl-Nielsen stain (auramine-rhodamine or resistance stain) is carried out. First, carbolic fuchsin or auramine is applied, then heat is applied and then a mixture of acid and alcohol is added, which act as bleaches, using methylene blue as a contrast dye.
Technique basis
The technique is based on the so-called acid-alcohol resistance. Mycobacteria contain a high content of lipids, including mycolic acids in the cell wall, which allow them to fix the carbolic fuchsin or auramine in their cell wall and to continue to retain it, even after the application of a mixture of acid and alcohol.
By staining the sample with basic fuchsin, the bacteria take on a reddish coloration, and by adding the acidic alcohol, the lipids of the bacteria resist the discoloration. This is why they are called acid-fast bacilli (ARB).
When looking at the slide under a microscope, small fuchsia-red rods are observed on a bluish background. Depending on the staining used, if smears are made with auramine-O staining, these yellow-green fluorescent rods will be observed on a dark background.
BAAR count
The smear is systematically traversed, observing each field of the microscope on the surface and in depth with 10x and 100x lenses (with immersion oil) and the number of BAARs observed in each field are noted. Then, an average of bacilli present is obtained.
It takes approximately 5 minutes to read 100 fields.
How is smear microscopy reported?
At an international level, the following report has been adopted using the Ziehl-Neelsen technique:
- When BAAR is not observed in 100 microscopic fields, it is reported as such: “acid-fast bacilli are not observed.“
- 1 to 9 BAAR in 100 fields: the total number of BAAR found in 100 fields is reported.
- 10 to 99 BAAR in 100 fields: positive (+) is reported.
- 1 to 10 BAAR in 50 fields: positive (++) is reported.
- More than 10 BAAR in 20 fields: positive (+++) is reported.
So if the smear test is positive (+, ++, +++) it means that the patient has TB.
If the smear microscopy reports less than 5 AFB in 100 fields, it’s recommended to extend the reading to 200 fields, perform a PCR test, and use a culture in liquid medium.
The reading and reporting of results of fluorescence-stained sheets has also been established internationally.
If possible, the results should be returned to the health center, within 24 hours of the laboratory receiving the samples.
Quality of smears
To ensure the quality of smears, each laboratory should ensure they do the following:
- Follow the stipulated rules for the proper use of the material, and thus avoid contamination.
- Have proper management of laboratory residues and wastes.
- Internal quality assessment (monitoring of performance indicators).
- External quality assessment (efficiency tests).
How to make smear microscopy a good control tool?
- This is achieved through adequate technical quality and maintaining adequate quality of laboratory records and reports.
- All laboratory services must be integrated into a National Network of Tuberculosis Laboratories and involve public and private laboratories in order to complement each other between the services.
- Procedures must be standardized (periodically reviewed by the Pan American Health Organization (PAHO), World Health Organization (WHO), and the International Union Against Tuberculosis and Respiratory Diseases (LA UNION).
Sensitivity and specificity of smear microscopy
Smear microscopy has a low sensitivity (40-60%) and a very high specificity. Smear microscopy has even lower sensitivity in cases of extrapulmonary disease, children, and patients with HIV / AIDS.
Smear microscopy, present and future
Ziehl-Nielsen staining (smear microscopy) has been the most widely-used technique for the past 100 years, as it requires simpler training.
In TB-endemic countries, a positive smear microscopy of a respiratory sample in an immunocompetent patient has a high predictive value. In other words, the risk of making a mistake when diagnosing the disease is very low.
The laboratory workers who process the samples must always observe the recommended biosafety measures and systematize the activities in order to reduce the risk of contagion.
The risk of contracting tuberculosis increases with the increase in the number of cases in a community, so early diagnosis is essential, with smear microscopy (BK) being a fundamental tool.
New emerging techniques are mercury lamp fluorescence microscopy and, for 10 years, the WHO has recommended the use of LED lamp fluorescence microscopy.
The latter is more sensitive, a totally dark room isn’t needed to read the smears, the reading time is reduced by almost half, and there’s less risk of contamination. However, staff need adequate training.
- Manual para el Diagnóstico Bacteriológico de la Tuberculosis. Parte 1: Manual de Actualización de la Baciloscopia/ Programa “Fortalecimiento de la Red de Laboratorios de Tuberculosis en la Región de las Américas”. Organización Panamericana de la Salud (PAHO); Organización Mundial de la Salud (OMS); COMISCA; Sistema de la Integración Centroamericana (SICA). 2da Edición. 2018. 88 p.
- Ramonda P Pino P, Cantillana P. Formularios de baciloscopia: ¿son un instrumento adecuado para el diagnóstico oportuno y seguimiento de la tuberculosis? Rev Chil Enf Respir 2014; 30: 103-110
- Polo C, Zabaleta A. Guía para la vigilancia por laboratorio de tuberculosis. Instituto Nacional de Salud, Colombia. 2020; 1-54.
- Betancourt J, Ruiz N, Cruces P, Velásquez, W. Sensibilidad de los métodos baciloscopia, cultivo y ELISA para el diagnóstico de la tuberculosis pulmonar, en pacientes del Edo. Vargas- Venezuela. Kasmera 30(2): 137-144, 2002
- cdc. gov. Centros para el Control y la Prevención de Enfermedades (CDC). Preguntas y respuestas sobre la tuberculosis. 2021; 1-24. Disponible en: http://www.cdc.gov/tb/esp.
Este texto se ofrece únicamente con propósitos informativos y no reemplaza la consulta con un profesional. Ante dudas, consulta a tu especialista.







