Insomnia and Other Sleep Disorders

Escrito y verificado por el psicólogo Bernardo Peña
Insomnia is a sleep disorder characterized by the inability to get a good night’s sleep. There are several types of insomnia, as well as other sleep disorders that are closely related.
The causes of insomnia, and sleep problems in general, can be both genetic and environmental. In this article, you’ll discover what sleep is and why it’s is essential, as well as the main sleep disorders.
Insomnia, why is it necessary to sleep?
The waking state is one in which one is awake or “vigilant”, where the subject is totally conscious and has a high interaction with the environment. Sleep, on the other hand, is a physiological state of low consciousness. Unlike coma or hibernation, sleep will recur and can quickly reverse.
The transition that occurs from wakefulness to sleep is known as the “circadian cycle or rhythm” and takes 24 hours to complete. Sleep, like appetite and sex, are basic functions of life. However, they can be altered by physical and mental factors, which will result in sleep disorders.

Why is insomnia so disturbing and sleep so necessary in life? Quite simply, this is because sleep helps to:
- Physiologically and metabolically recover the different systems in the body
- Reestablish the balance of neuronal excitation
- Reorganize the information that has been obtained during the day relating it to long-term memory
- Delete irrelevant information so as not to overload memory
- Restore lost energy
- Consolidate what you have learned during the day
It’s impossible for someone to go without sleep for a long time because they would die. And whether it occurs totally or partially, the person will experience different psychopathological manifestations.
- If there’s a sleep deprivation for 60 to 200 hours the person may experience:
- Drowsiness
- Decreased performance: reduced ability to concentrate, perseverance in tasks, and verbal communication
- Changes in mood
- If sleep deprivation is greater than 200 hours the person will have:
- Microdreams
- Allopsychic disorientation
- Paranoid delusions
- Delusions
- Hallucinations
Electrophysiological characteristics of sleep
In sleep, 5 physiological levels have been distinguished by polysomnography. These are non-REM sleep (with its 4 subphases) and REM sleep.
The acronym REM stands for rapid eye movement. These will refer to the presence or absence of eye movements in the different phases of sleep.
Non-REM sleep
It lasts 45 to 60 minutes from the start of Phase I to the end of Phase IV. Its total percentage, in relation to sleep, will be 75%. Being 5% Phase I, 45% Phase II, 12% Phase II, and 13% Phase IV. In humans, there are three phases that comprise non-REM sleep, which are:
Non-REM sleep phase I
This first stage consists of the transition from the waking state to the beginning of sleep. It can last from a few seconds to about 10 minutes. It’s characterized by the gradual disappearance of alpha waves, typical of waking states. These waves, from 8 to 12 cycles per second, begin to be replaced by beta waves, whose voltage is higher, around 4 to 7 cycles per second.
In turn, tonic activity decreases and slow eye movements occur. During this state, sleep can be easily interrupted. During this period the subject can frequently return to the waking state before moving on to phase II.
Phase II non-REM sleep
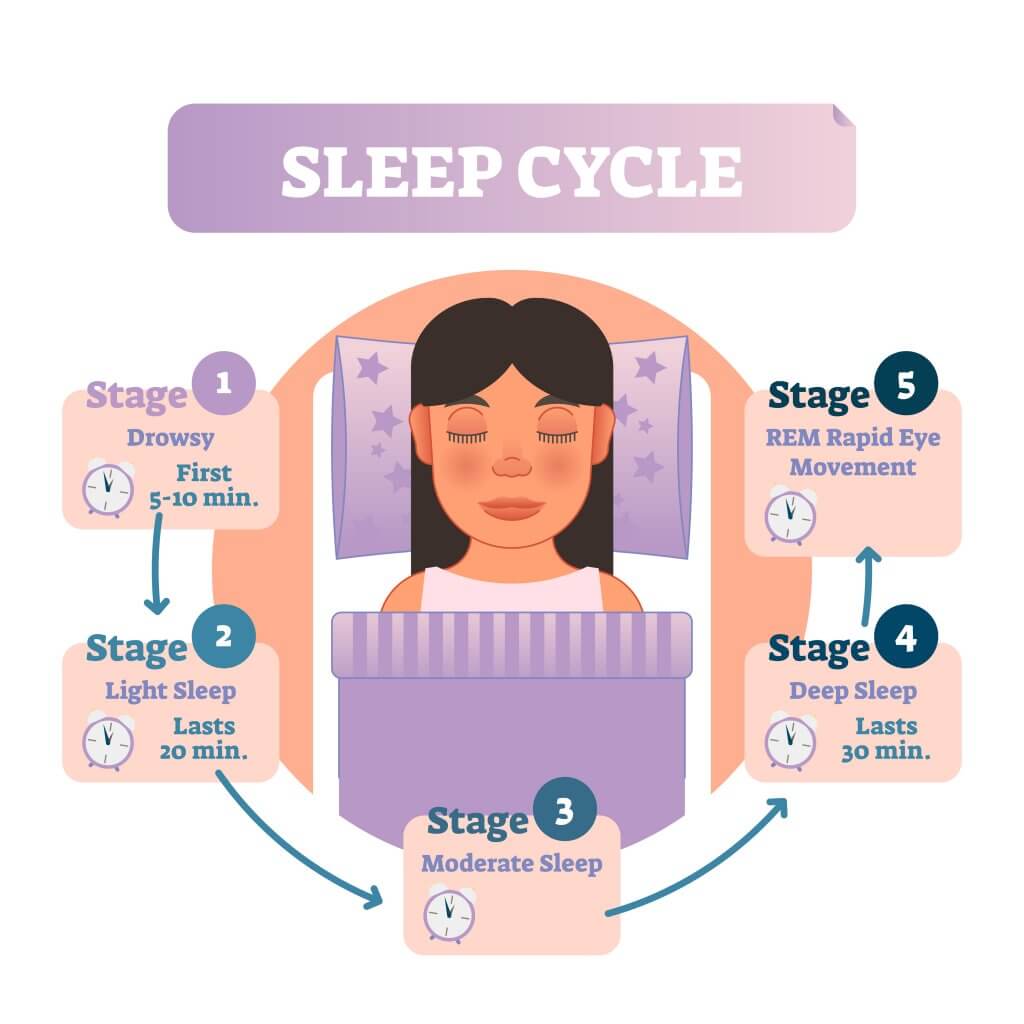
This phase occurs 5 or 10 minutes after phase I. In fact, these two phases together are known as light sleep.
Its activity is of low voltage and frequencies similar to phase I. However, two phenomena that characterize it appear: sleep spindles and K complexes. Sleep spindles are 12-14Hz waves that appear with a frequency of 3 to 8 min and the K complexes are high-voltage bipolar waves that appear suddenly.
During this phase, the threshold for awakening rises. That’s why a stimulus that would have awakened the person in Phase I may not awaken them in Phase II.
Its appearance is usually considered a sign that the subject is finally sleeping. As for the tonic activity, it decreases even more. In fact, eye movements almost completely disappear.
Phases III and IV of non-REM sleep
In this phase, the delta and theta rhythms predominate. It’s said that, when the trace is formed between 20% and 50% by delta waves, it has already passed to phase III. These waves have a voltage up to 100W, and a frequency of 1 to 3 cycles per second.
Sleep spindles also appear sporadically in this phase and there’s an even more significant decrease in muscle tone. On the other hand, breathing is held regularly and blood pressure begins to drop. To be able to wake up a subject in this state, a strong sound stimulation would be needed.

Phase IV is a deeper stage. The EGG pattern is going to be the same as phase III, but now, at least 50% are delta waves. This phase, together with the previous one, constitutes the so-called deep sleep. At this stage, sleep spindles and K complexes will no longer appear.
The person will have greater difficulty waking up to stimuli, but if they succeed, their response will be clumsy and slow. In addition, muscle atony appears and the respiratory rate decreases again. This phase is going to be difficult to achieve in people who suffer from insomnia and other sleep disorders, such as sleepwalking and night terrors.
REM sleep
This phase is called REM because it’s characterized by the presence of rapid eye movements.
The first REM period begins 90 minutes after reaching all the states previously mentioned. In addition, it’s equivalent to 25% of the person’s total sleep. Its layout has an electrical similarity to phase I. However, this is going to appear somewhat faster.
Alpha and beta rhythms, heart rate, respiratory rate, and blood pressure will be similar to those of the waking phase. However, there’ll be a complete nullification of muscle tone with sporadic contractions of the hands or face.
During the REM phase, the person will experience abstract and surreal daydreams. In most cases, people who wake up during this phase will vividly remember what they were dreaming about.
Sleep disturbances
These are divided into two large groups: dysomnias and parasomnias.
Dysomnias
This category is related to the duration, intensity, and amount of sleep. Within it, we have insomnia, hypersomnia, and narcolepsy.
Insomnia
Insomnia is a sleep disturbance that involves difficulty starting or staying asleep. Once the person wakes up they’ll be unable to go back to sleep, but it will be difficult for them to be fresh and active in the morning.

For a person to be diagnosed with insomnia disorder, they must meet the following characteristics:
- It happens at least 3 nights a week and for 3 months
- It must be ruled out that it’s secondary to some other sleep disorder
- It mustn’t be related to the use of a substance
- It can’t be explained by mental or medical disorders.
In general, people with insomnia have bad or unhealthy routines that affect the quality and quantity of their sleep. There can also be outside influences. For example:
- Irregular hours
- Eating out a lot
- Consuming alcohol before sleeping
- Doing strenuous exercise at night
- Going to bed too early
- Doing jobs or activities that require high brain stimulation at night
- Taking stimulating drinks or substances before going to bed
- Living in areas with a lot of noise
- When the ambient temperature is extreme
- They’re in a stressful situation

Some of the consequences of insomnia would be:
- Functional impairment
- Loss of productivity
- Attention problems
- Memory impairment
- Less ability to relate on an interpersonal level
- Alterations in mood
- Hormonal and metabolic problems
- Stunted growth
- Early aging
- Weight gain
Primary insomnia
This type of insomnia is characterized by the fact that a particular cause cannot be attributed with certainty. However, it’s believed that stress could be a trigger. In many cases it arises in childhood and can be prolonged throughout life, increasing with age.
The symptoms that the subjects will have will be fatigue, tiredness, headaches, muscular tension and gastric discomfort. The reason why this type of insomnia is prolonged is that the subject is constantly worried about their state, which makes it difficult for them to fall asleep at night.

Because of this, a state of anxiety and tension develops during the day that causes a sleep disturbance at night. This disorder can also cause daytime hypersomnia.
Hypersomnia
Hypersomnia is characterized by excessive sleepiness that can be nocturnal (greater than or equal to 10 hours) or daytime (frequent naps that can last more than 1 hour). It usually begins around 15 and 35 years of age, and tends to become chronic.
For this to be considered a disorder, it must occur for at least 1 month. In addition, it mustn’t be associated with another medical disorder or the effects of a substance. Also, narcolepsy should be ruled out.
Patients suffering from this disorder may fall asleep during the day, but their sleep isn’t going to be restful. Its symptoms will be low level of alertness, performance, and concentration. This may have repercussions in the person’s work and social environment, in addition to being involved in accidents or major distractions, due to a lack of attention and concentration.
Narcolepsy
Narcolepsy is a syndrome of unknown origin characterized by abnormal sleep attacks. It usually begins in adolescence, but is consolidated in the person around the age of 25. Narcolepsy is made up of four symptoms that form the narcoleptic tetrad. Drowsiness is the most frequent symptom.

- Excessive daytime sleepiness: Patients experience acute sleep attacks during circumstances that could be considered stimulating. This episode lasts between 10 and 15 minutes, and there’s usually a refractory period of several hours before the next episode.
- Cataplexy: This is an alteration of the psychomotor skills due to suddenly entering the REM phase. The person will experience a sudden decrease in muscle tone, and will be fully aware of it. It will usually be triggered by intense emotions such as laughing, crying, or anger. Generally, it lasts a few seconds. These episodes will start years after daytime sleepiness sets in.
- Sleep paralysis: This is a similar state to cataplexy. The patient is conscious but feels unable to move, speak, or breathe naturally. The difference is that it doesn’t have emotional triggers. Its duration will be no longer than a few minutes, and can stop earlier if there are external stimuli.
- Hypnagogic hallucinations: Hallucinogenic episodes are auditory or visual pseudoperceptions. Generally, they won’t appear until adolescence, and they’ll tend to decrease over time. There are cases in which paralysis and hallucinations occur simultaneously, and this is terrifying for the patient.
Breathing-related sleep disorders
Sleep apnea syndrome is a breathing disorder characterized by the repetitive interruption (more than 10 seconds) of the naso-buccal airflow during sleep. From polysomnographic studies, three types of apneas can be distinguished: obstructive, central and mixed.
Obstructive sleep apnea
This consists of the cessation of airflow, which starts again suddenly. This is the most common apnea. During sleep, the muscles relax and the airways narrow so that breathing becomes insufficient for 10 to 20 seconds.

The brain detects this abnormality and awakens the person. The most characteristic sign will be snoring, as the walls of the throat cave inwards.
As this respiratory cessation will occur throughout the night, the person won’t be able to enter phases III and IV of sleep, and will be a non-restorative sleep. On the other hand, there won’t be an adequate exchange of gases, causing different degrees of nocturnal hypoxemia and hypercapnia.
Central sleep apnea
This consists of the partial cessation of the respiratory rhythm due to the efferent neurons of the brain preventing the muscles that control respiration from acting correctly. This will only happen in cases where the Central Nervous System (CNS) has been damaged.
Mixed sleep apnea
This is the combination of the two apneas mentioned above. Sometimes the respiratory system will be paralyzed and other times there’ll be an obstruction of the airways.
Circadian rhythm disorders
These are sleep disturbances due to a disorganization of sleep-wakefulness. That means that the person sleeps the corresponding hours, but the sleep schedules are altered. Humans are governed by circadian rhythms, which are linked to temperature, genetics, and exposure to light.
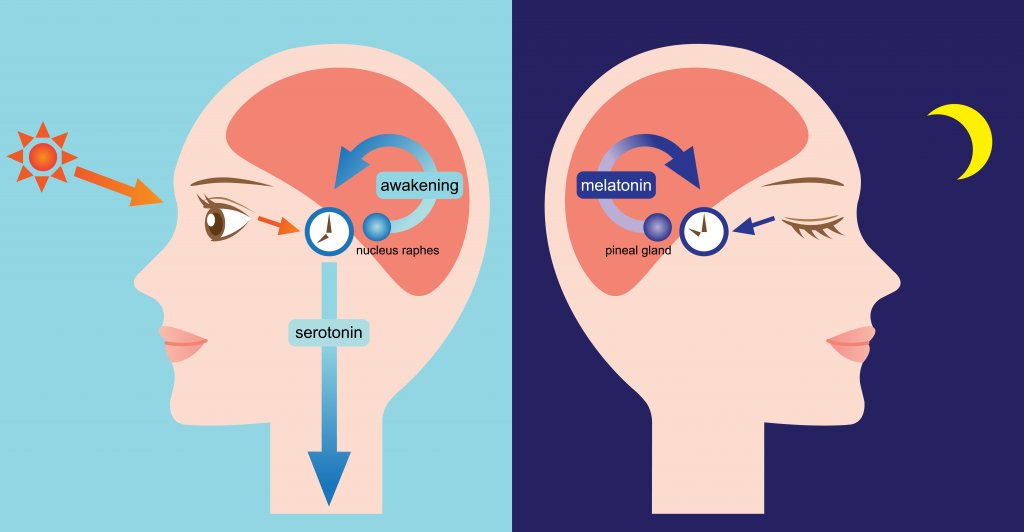
In addition, the body has a hormone called melatonin that is released during the night and is what induces sleep. All these elements will govern the patterns which cause the person to wake and fall asleep. Within this group, we find the following disorders:
- Delayed sleep phases: These arise from a delay in going to sleep (more than 2 hours)
- Advanced sleep phases: Circadian biomarkers have been programmed 2 to 4 hours earlier than usual, as the person has become accustomed to getting up early.
- Associated with work shifts: This happens to people who have unusual work hours. For example, one week they work at night and the other week they work during the morning. This interferes with them maintaining a normal sleep-wake schedule.
Parasomnias
Parasomnias are abnormalities that occur in the REM and NON-REM phases of sleep.
Nightmares
Nightmares are episodes that occur during REM sleep. They have to do with the situations that the person is dreaming of, which can be terrifying, distressing, or threatening.
Anxiety can provoke a motor reaction that awakens the person. However, this anxiety will dissipate as soon as you realize that you were only dreaming and that the situation isn’t real.

Nightmares can be experienced regardless of age, although they’re more common in children. Its etiology isn’t known exactly, but some theories say that they have an important meaning for the person.
Night terrors
Night terrors usually occur in stages III or IV of sleep. That is, during the deepest sleep. They begin with a heartbreaking scream in the middle of the night.
Generally, the person will wake up with a diffuse distressing sensation, without knowing exactly what has happened or remembering anything. Its etiology is believed to be related to emotional stress and fatigue.
Somnambulism
Sleepwalking is characterized by a sequence of body movements that the person performs during slow-wave sleep. The person may get up and perform various activities such as walking around the house or moving things.

The person could even utter a few words. During this state, the person doesn’t react to environmental stimuli. Its duration can be from 1 to 30 minutes and it can occur several times a week throughout life. Its cause remains unknown, but some researchers associate it with stress.
Conclusions about insomnia and other sleep disorders
In conclusion, in this article we’ve seen what sleep is, its importance, and its main characteristics. On the other hand, we have seen the consequences of sleep deprivation, or suffering from insomnia. Likewise, we have seen the most common sleep disorders that are related to insomnia.
If you suffer from any of these symptoms, we recommend you go to a doctor or psychologist to treat both insomnia and other sleep disorders. Today there are excellent psychological and pharmacological therapies that offer increasingly better results.
Insomnia is a sleep disorder characterized by the inability to get a good night’s sleep. There are several types of insomnia, as well as other sleep disorders that are closely related.
The causes of insomnia, and sleep problems in general, can be both genetic and environmental. In this article, you’ll discover what sleep is and why it’s is essential, as well as the main sleep disorders.
Insomnia, why is it necessary to sleep?
The waking state is one in which one is awake or “vigilant”, where the subject is totally conscious and has a high interaction with the environment. Sleep, on the other hand, is a physiological state of low consciousness. Unlike coma or hibernation, sleep will recur and can quickly reverse.
The transition that occurs from wakefulness to sleep is known as the “circadian cycle or rhythm” and takes 24 hours to complete. Sleep, like appetite and sex, are basic functions of life. However, they can be altered by physical and mental factors, which will result in sleep disorders.
Why is insomnia so disturbing and sleep so necessary in life? Quite simply, this is because sleep helps to:
- Physiologically and metabolically recover the different systems in the body
- Reestablish the balance of neuronal excitation
- Reorganize the information that has been obtained during the day relating it to long-term memory
- Delete irrelevant information so as not to overload memory
- Restore lost energy
- Consolidate what you have learned during the day
It’s impossible for someone to go without sleep for a long time because they would die. And whether it occurs totally or partially, the person will experience different psychopathological manifestations.
- If there’s a sleep deprivation for 60 to 200 hours the person may experience:
- Drowsiness
- Decreased performance: reduced ability to concentrate, perseverance in tasks, and verbal communication
- Changes in mood
- If sleep deprivation is greater than 200 hours the person will have:
- Microdreams
- Allopsychic disorientation
- Paranoid delusions
- Delusions
- Hallucinations
Electrophysiological characteristics of sleep
In sleep, 5 physiological levels have been distinguished by polysomnography. These are non-REM sleep (with its 4 subphases) and REM sleep.
The acronym REM stands for rapid eye movement. These will refer to the presence or absence of eye movements in the different phases of sleep.
Non-REM sleep
It lasts 45 to 60 minutes from the start of Phase I to the end of Phase IV. Its total percentage, in relation to sleep, will be 75%. Being 5% Phase I, 45% Phase II, 12% Phase II, and 13% Phase IV. In humans, there are three phases that comprise non-REM sleep, which are:
Non-REM sleep phase I
This first stage consists of the transition from the waking state to the beginning of sleep. It can last from a few seconds to about 10 minutes. It’s characterized by the gradual disappearance of alpha waves, typical of waking states. These waves, from 8 to 12 cycles per second, begin to be replaced by beta waves, whose voltage is higher, around 4 to 7 cycles per second.
In turn, tonic activity decreases and slow eye movements occur. During this state, sleep can be easily interrupted. During this period the subject can frequently return to the waking state before moving on to phase II.
Phase II non-REM sleep
This phase occurs 5 or 10 minutes after phase I. In fact, these two phases together are known as light sleep.
Its activity is of low voltage and frequencies similar to phase I. However, two phenomena that characterize it appear: sleep spindles and K complexes. Sleep spindles are 12-14Hz waves that appear with a frequency of 3 to 8 min and the K complexes are high-voltage bipolar waves that appear suddenly.
During this phase, the threshold for awakening rises. That’s why a stimulus that would have awakened the person in Phase I may not awaken them in Phase II.
Its appearance is usually considered a sign that the subject is finally sleeping. As for the tonic activity, it decreases even more. In fact, eye movements almost completely disappear.
Phases III and IV of non-REM sleep
In this phase, the delta and theta rhythms predominate. It’s said that, when the trace is formed between 20% and 50% by delta waves, it has already passed to phase III. These waves have a voltage up to 100W, and a frequency of 1 to 3 cycles per second.
Sleep spindles also appear sporadically in this phase and there’s an even more significant decrease in muscle tone. On the other hand, breathing is held regularly and blood pressure begins to drop. To be able to wake up a subject in this state, a strong sound stimulation would be needed.
Phase IV is a deeper stage. The EGG pattern is going to be the same as phase III, but now, at least 50% are delta waves. This phase, together with the previous one, constitutes the so-called deep sleep. At this stage, sleep spindles and K complexes will no longer appear.
The person will have greater difficulty waking up to stimuli, but if they succeed, their response will be clumsy and slow. In addition, muscle atony appears and the respiratory rate decreases again. This phase is going to be difficult to achieve in people who suffer from insomnia and other sleep disorders, such as sleepwalking and night terrors.
REM sleep
This phase is called REM because it’s characterized by the presence of rapid eye movements.
The first REM period begins 90 minutes after reaching all the states previously mentioned. In addition, it’s equivalent to 25% of the person’s total sleep. Its layout has an electrical similarity to phase I. However, this is going to appear somewhat faster.
Alpha and beta rhythms, heart rate, respiratory rate, and blood pressure will be similar to those of the waking phase. However, there’ll be a complete nullification of muscle tone with sporadic contractions of the hands or face.
During the REM phase, the person will experience abstract and surreal daydreams. In most cases, people who wake up during this phase will vividly remember what they were dreaming about.
Sleep disturbances
These are divided into two large groups: dysomnias and parasomnias.
Dysomnias
This category is related to the duration, intensity, and amount of sleep. Within it, we have insomnia, hypersomnia, and narcolepsy.
Insomnia
Insomnia is a sleep disturbance that involves difficulty starting or staying asleep. Once the person wakes up they’ll be unable to go back to sleep, but it will be difficult for them to be fresh and active in the morning.
For a person to be diagnosed with insomnia disorder, they must meet the following characteristics:
- It happens at least 3 nights a week and for 3 months
- It must be ruled out that it’s secondary to some other sleep disorder
- It mustn’t be related to the use of a substance
- It can’t be explained by mental or medical disorders.
In general, people with insomnia have bad or unhealthy routines that affect the quality and quantity of their sleep. There can also be outside influences. For example:
- Irregular hours
- Eating out a lot
- Consuming alcohol before sleeping
- Doing strenuous exercise at night
- Going to bed too early
- Doing jobs or activities that require high brain stimulation at night
- Taking stimulating drinks or substances before going to bed
- Living in areas with a lot of noise
- When the ambient temperature is extreme
- They’re in a stressful situation
Some of the consequences of insomnia would be:
- Functional impairment
- Loss of productivity
- Attention problems
- Memory impairment
- Less ability to relate on an interpersonal level
- Alterations in mood
- Hormonal and metabolic problems
- Stunted growth
- Early aging
- Weight gain
Primary insomnia
This type of insomnia is characterized by the fact that a particular cause cannot be attributed with certainty. However, it’s believed that stress could be a trigger. In many cases it arises in childhood and can be prolonged throughout life, increasing with age.
The symptoms that the subjects will have will be fatigue, tiredness, headaches, muscular tension and gastric discomfort. The reason why this type of insomnia is prolonged is that the subject is constantly worried about their state, which makes it difficult for them to fall asleep at night.
Because of this, a state of anxiety and tension develops during the day that causes a sleep disturbance at night. This disorder can also cause daytime hypersomnia.
Hypersomnia
Hypersomnia is characterized by excessive sleepiness that can be nocturnal (greater than or equal to 10 hours) or daytime (frequent naps that can last more than 1 hour). It usually begins around 15 and 35 years of age, and tends to become chronic.
For this to be considered a disorder, it must occur for at least 1 month. In addition, it mustn’t be associated with another medical disorder or the effects of a substance. Also, narcolepsy should be ruled out.
Patients suffering from this disorder may fall asleep during the day, but their sleep isn’t going to be restful. Its symptoms will be low level of alertness, performance, and concentration. This may have repercussions in the person’s work and social environment, in addition to being involved in accidents or major distractions, due to a lack of attention and concentration.
Narcolepsy
Narcolepsy is a syndrome of unknown origin characterized by abnormal sleep attacks. It usually begins in adolescence, but is consolidated in the person around the age of 25. Narcolepsy is made up of four symptoms that form the narcoleptic tetrad. Drowsiness is the most frequent symptom.
- Excessive daytime sleepiness: Patients experience acute sleep attacks during circumstances that could be considered stimulating. This episode lasts between 10 and 15 minutes, and there’s usually a refractory period of several hours before the next episode.
- Cataplexy: This is an alteration of the psychomotor skills due to suddenly entering the REM phase. The person will experience a sudden decrease in muscle tone, and will be fully aware of it. It will usually be triggered by intense emotions such as laughing, crying, or anger. Generally, it lasts a few seconds. These episodes will start years after daytime sleepiness sets in.
- Sleep paralysis: This is a similar state to cataplexy. The patient is conscious but feels unable to move, speak, or breathe naturally. The difference is that it doesn’t have emotional triggers. Its duration will be no longer than a few minutes, and can stop earlier if there are external stimuli.
- Hypnagogic hallucinations: Hallucinogenic episodes are auditory or visual pseudoperceptions. Generally, they won’t appear until adolescence, and they’ll tend to decrease over time. There are cases in which paralysis and hallucinations occur simultaneously, and this is terrifying for the patient.
Breathing-related sleep disorders
Sleep apnea syndrome is a breathing disorder characterized by the repetitive interruption (more than 10 seconds) of the naso-buccal airflow during sleep. From polysomnographic studies, three types of apneas can be distinguished: obstructive, central and mixed.
Obstructive sleep apnea
This consists of the cessation of airflow, which starts again suddenly. This is the most common apnea. During sleep, the muscles relax and the airways narrow so that breathing becomes insufficient for 10 to 20 seconds.
The brain detects this abnormality and awakens the person. The most characteristic sign will be snoring, as the walls of the throat cave inwards.
As this respiratory cessation will occur throughout the night, the person won’t be able to enter phases III and IV of sleep, and will be a non-restorative sleep. On the other hand, there won’t be an adequate exchange of gases, causing different degrees of nocturnal hypoxemia and hypercapnia.
Central sleep apnea
This consists of the partial cessation of the respiratory rhythm due to the efferent neurons of the brain preventing the muscles that control respiration from acting correctly. This will only happen in cases where the Central Nervous System (CNS) has been damaged.
Mixed sleep apnea
This is the combination of the two apneas mentioned above. Sometimes the respiratory system will be paralyzed and other times there’ll be an obstruction of the airways.
Circadian rhythm disorders
These are sleep disturbances due to a disorganization of sleep-wakefulness. That means that the person sleeps the corresponding hours, but the sleep schedules are altered. Humans are governed by circadian rhythms, which are linked to temperature, genetics, and exposure to light.
In addition, the body has a hormone called melatonin that is released during the night and is what induces sleep. All these elements will govern the patterns which cause the person to wake and fall asleep. Within this group, we find the following disorders:
- Delayed sleep phases: These arise from a delay in going to sleep (more than 2 hours)
- Advanced sleep phases: Circadian biomarkers have been programmed 2 to 4 hours earlier than usual, as the person has become accustomed to getting up early.
- Associated with work shifts: This happens to people who have unusual work hours. For example, one week they work at night and the other week they work during the morning. This interferes with them maintaining a normal sleep-wake schedule.
Parasomnias
Parasomnias are abnormalities that occur in the REM and NON-REM phases of sleep.
Nightmares
Nightmares are episodes that occur during REM sleep. They have to do with the situations that the person is dreaming of, which can be terrifying, distressing, or threatening.
Anxiety can provoke a motor reaction that awakens the person. However, this anxiety will dissipate as soon as you realize that you were only dreaming and that the situation isn’t real.
Nightmares can be experienced regardless of age, although they’re more common in children. Its etiology isn’t known exactly, but some theories say that they have an important meaning for the person.
Night terrors
Night terrors usually occur in stages III or IV of sleep. That is, during the deepest sleep. They begin with a heartbreaking scream in the middle of the night.
Generally, the person will wake up with a diffuse distressing sensation, without knowing exactly what has happened or remembering anything. Its etiology is believed to be related to emotional stress and fatigue.
Somnambulism
Sleepwalking is characterized by a sequence of body movements that the person performs during slow-wave sleep. The person may get up and perform various activities such as walking around the house or moving things.
The person could even utter a few words. During this state, the person doesn’t react to environmental stimuli. Its duration can be from 1 to 30 minutes and it can occur several times a week throughout life. Its cause remains unknown, but some researchers associate it with stress.
Conclusions about insomnia and other sleep disorders
In conclusion, in this article we’ve seen what sleep is, its importance, and its main characteristics. On the other hand, we have seen the consequences of sleep deprivation, or suffering from insomnia. Likewise, we have seen the most common sleep disorders that are related to insomnia.
If you suffer from any of these symptoms, we recommend you go to a doctor or psychologist to treat both insomnia and other sleep disorders. Today there are excellent psychological and pharmacological therapies that offer increasingly better results.
- Contreras, A. “Insomnio: generalidades y alternativas terapéuticas de última generación.” Revista Médica Clínica Las Condes 24.3 (2013): 433-441.
- Peña-Herrera, B. (2018) Psicopatología General. Samborondón: Universidad Espíritu Santo – Ecuador.
- Romero, O., T. Sagalés, and M. J. Jurado. “Insomnio: diagnóstico, manejo y tratamiento.” Rev. Med Univ Navarra 49.1 (2005): 25-30.
- Sarrais, F., and P. de Castro Manglano. “El insomnio.” Anales del sistema sanitario de Navarra. Vol. 30. Gobierno de Navarra. Departamento de Salud, 2007.
Este texto se ofrece únicamente con propósitos informativos y no reemplaza la consulta con un profesional. Ante dudas, consulta a tu especialista.







