What Are Antibiotics?

Antibiotics are chemical substances produced by a living being, or synthetic derivatives of them that kill or prevent the growth of certain classes of sensitive microorganisms. Generally, they’re drugs used in the treatment of bacterial infections. That’s why they’re known as antibacterials, and are used in human and animal medicine.
They generally help the person or animal’s defenses until local responses are able to control the infection. The objective of antibiotic treatment is to achieve the eradication of the pathogenic or bacterial microorganism.
In order to do this, it’s necessary to follow a dosage that achieves a drug concentration higher than the minimum concentration – one that’s capable of interfering with the proliferation of the microorganism involved in the infection. However, self-medication with antibiotics is a serious public health problem, and we’ll talk about it a bit later in the article.
The history of antibiotics
The first antibiotic was penicillin and was discovered in 1897 by Ernest Duchesne, in France. The scientist worked with fungi of the genus Penicillium. However, his work didn’t receive the attention of the scientific community.
Later on, Alexander Fleming, a British physician, was growing the Staphylococcus aureus bacteria on a petri dish. The culture was accidentally contaminated by fungi, and, as a result, he noticed that the growth around the mold was free of bacteria.
Although he couldn’t purify the material obtained, he published the discovery in the scientific literature. Since the fungus was of the genus Penicillium, the substance that interfered with this bacterial growth would be called penicillin.
The discovery of antibiotics, like other important discoveries such as anesthesia or the adoption of hygienic practices, revolutionized medicine and became one of the great advances in the history of medicine. Next, we’ll look at the following points about antibiotics:
- Classes of antibiotics
- Classification
- Antibiotic resistance
Classes of antibiotics
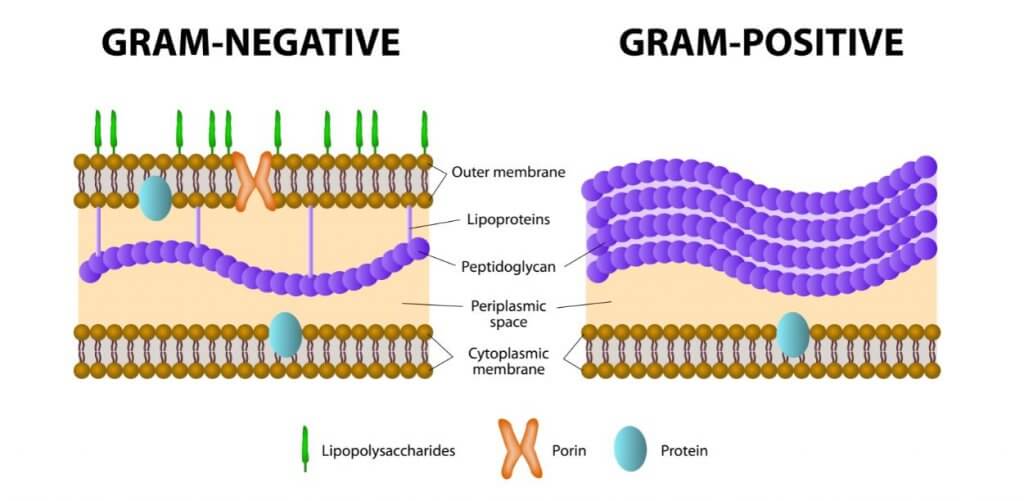
Unlike the previous ones, Gram – bacteria have a more complex cell wall. They have an inner cell wall, a peptidoglycan wall, and an outer lipid bilayer. To find out if a bacterium is Gram + or Gram – Gram staining is performed in the laboratory.
Those with a positive sign will turn blue or purple, while those with a negative sign will turn red. In this sense, narrow-spectrum antibiotics are only effective against one type of bacteria, either Gram + or Gram -.
On the contrary, broad-spectrum ones are effective against both types of bacteria. In addition to this type of antibiotic, it’s necessary to differentiate between those that are bacteriostatic and those that are bactericidal. The former are those that inhibit the growth of the microorganism without inducing its death. On the other hand, bactericides do induce the death of the bacteria. Some bacteriostatic antibiotics can be considered bactericidal above a certain concentration.
Classification
The classification of these drugs is established according to the mechanism of action they trigger. Thus, we can find the following drugs:
1. Inhibitors of cell wall synthesis
Bacteria of the Mycoplasma, Chlamydia and Rickettsia genera don’t have a cell wall, and so they’re resistant to this type of antibiotic. Within this group, we differentiate between beta-lactams, glucopectidics, and bacitracin A.
a) Beta-lactams
They’re narrow-spectrum drugs, since they’re only effective against Gram + bacteria; in addition, they’re bactericidal. These medications are administered orally and parenterally. In addition, they’re very safe drugs as the possible adverse reactions are just limited to possible allergic reactions.
They can penetrate the placenta, but, despite this, they can still be used during pregnancy. They’re used for all kinds of infections, and, among the most common, we can find:
- Penicillin
- Cephalosporins
- Monobactams (active against Gram – bacteria)
- Carbapenems
b) Glycopeptides
These antibiotics inhibit the synthesis of the cell wall from the outside, and they’re also bactericidal. Their main characteristic is that they reduce the resistance that bacteria can develop, and ensure the effectiveness of other antibiotics.
They facilitate the reduction of the peptidoglycan framework of Gram – bacteria. Because of this, they favor the action of specific drugs against these bacteria. However, glycopeptides are particularly effective against Gram + bacteria.
A typical pharmacological combination is the administration of aminoglycosides (which inhibit protein synthesis) with vancomycin, which favors the action of aminoglycosides. Vancomycin – the most representative drug in this group – is administered intravenously.
Caution must be exercised because it’s a drug with a high toxicity, and, if the infusion is too quick, then the patient may suffer from red neck syndrome. It can also be given orally, but only for the treatment of pseudomembranous colitis. If administered intravenously, the main indication is to treat infections resistant to penicillins and cephalosporins, or people allergic to the latter.
c) Bacitracin A
This drug inhibits the regeneration of peptidoglycan transporter lipid. It has a narrow spectrum, as it’s only effective against infections by Gram + bacteria. It’s administered topically, as the intramuscular route is very painful, and it presents a lot of toxicity intravenously. For this reason, it’s used in eye, skin, and throat infections.
2. Interference with membrane function

Thus, the components of the cell leave and cell lysis occurs. They’re effective against Gram – and are administered topically. They’re often associated with bacitracin A or neomycin. As for Na colistemetate, its use is limited to hospitals, and it’s primarily used in respiratory infections and cystic fibrosis.
3. Inhibitors of protein synthesis

- Aminoglycosides
- Streptogramins
- Macrolides
- Lincosamides
- Tetracyclines
- Amphenicols
a) Aminoglycosides
Gentamicin is the most widely used. These antibiotics enter the cell by active transport. Upon reaching the cytoplasm, they irreversibly bind to the 30S subunit of ribosomes. In this way, they decrease protein synthesis or cause proteins to be synthesized as defective proteins. They’re active against Gram – bacteria.
Due to their low bioavailability, its use is limited to intravenous administration in hospitals. However, it can also be administered intramuscularly in an outpatient setting. The most serious adverse reactions are ototoxicity and nephrotoxicity. This is because these structures are similar to the cell membrane, and due to the fact that aminoglycosides bind and accumulate.
As a result, continuous use at high doses can cause deafness and kidney problems. The regimen of administration of these antibiotics is by rapid infusion, and for a short period of time so that it doesn’t accumulate, thus reducing adverse reactions. Its main use is for serious infections by Enterobacteriaceae and Pseudomonas aeruginosa.
b) Streptogramins
c) Macrolides
These antibiotics bind to the 50S subunit, inhibiting translocation. They’re bacteriostatic, although there are some with bactericidal action. They’re broad-spectrum, but are more effective against Gram +. Besides, they’re also a good alternative to penicillins. Erythromycin is the best option for pertussis. They’re also effective in treating respiratory infections and non-hospital pneumonia.
d) Lincosamides
These are also similar to macrolides. They’re systemically aggressive drugs because they cause pseudomembranous colitis. For this reason, it’s limited to topical use.
c) Tetracyclines
They enter the cell by passive diffusion because they’re very fat-soluble, and they can also use active transport coupled with some alterable transporter. On the other hand, oral absorption is regular, and decreases with the intake of food (it shouldn’t be taken with milk or dairy) and with divalent cations because they can form complexes.
They’re widely distributed throughout the body and have a high affinity for developing bones and teeth, and they can turn yellow or brown, especially in children. It’s worth mentioning that the most characteristic adverse reactions of these drugs affect the digestive system. These antibiotics are contraindicated in the gestation period, during lactation, and in children under 8 years of age.
d) Amphenicols
The most powerful antibiotic in this group is chloramphenicol. Its mechanism of action is that the drug enters the cell by facilitated diffusion to bind to the 50S subunit of its ribosomes. They inhibit the binding of aminoacyl tRNA and consequently inhibit protein synthesis and therefore bacterial proliferation.
For this reason, they’re bacteriostatic. If this process occurs in eukaryotic cells of the body, then toxicity will occur, especially in the bone marrow. Developed countries avoid using it and use others that are more expensive and safer.
Its administration is reduced as an alternative in people allergic to cephalosporins in bacterial meningitis and tetracyclines in cases of Rocky Mountain fever. In developing countries, the benefit is greater than the risk, which is why it is used primarily to treat enteric fever.
4. Inhibition of DNA synthesis
We can distinguish between two groups:
Quinolones and fluoroquinolones
The former are narrow-spectrum while the fluoroquinolones are broad-spectrum. They decrease the activity of the DNA gyrase. At high concentrations, the activity of topoisomerase II, both bacterial and human, also decreases, and so it could have some antineoplastic action. They’re used in infections of all kinds, as prophylactics in immunosuppressed people and in people who have resistance to tuberculosis.
Nitroimidazole
These are antibacterial, antifungal, and antiparasitic. Its activity requires 5′-nitro reduction by enzymes called nitroreductases. Intermediates are cytotoxic, thus reducing DNA synthesis. They’re bactericidal with reduced action because the enzymes necessary for these antibiotics to take effect are not found in all bacteria. It should be mentioned that metronidazole is mutagenic.
5. Inhibitors of RNA synthesis
This group is represented by rifampicins. They’re effective against mycobacteria, Gram + bacteria, and some Gram – bacteria. They’re used in the treatment of tuberculosis, and inhibit RNA synthesis by blocking RNA polymerase. Depending on the concentration administered, they’re bactericidal or bacteriostatic antibiotics. We can highlight 3 drugs from this group:
- Rifampicin: This is the most used in tuberculosis and leprosy. Produces hepatotoxicity.
- Rifaximin: This is an intestinal anti-infective.
- Rifabutin: Prevents Mycobacterium avium-intracellulare infections and is effective in difficult-to-treat infections – especially in immunosuppressed patients.
6. Inhibition of folic acid synthesis

a) Sulfamides
Sulfadiazine is the reference drug in this group, and inhibits the DHFS enzyme. One of its adverse reactions is allergy-related, and it’s administered topically and systemically. Bacteria can develop resistance to these drugs if they decrease the permeability of the cell membrane.
b) Sulfones
The most widely-used drug in this family is dapsone and it’s effective against the bacterium Mycobacterium leprae. It is, therefore, an antileprosy drug.
7. DHPR inhibitors
Within this group we can mention:
- Trimethoprim: This is a bacteriostatic which can be given alone or with sulfa drugs. It’s the choice option for acute and chronic urinary infections. It’s also used for respiratory infections, pneumonia, and gastroenteritis.
- Pyrimethamine: This is an antiparasitic, and is used for the treatment of malaria.
- Trimetexate: It inhibits DHFR in humans. For that reason, it inhibits the proliferation of eukaryotic, neoplastic, and immune cells. Therefore, it has an antineoplastic effect similar to that of methotrexate.
8. Anti-tuberculosis and anti-leprosy
Treatment tries to quickly control and kill the bacilli that cause the disease and also prevents or decreases the number of relapses. These are very long treatments with more than one active principle. The problem with this type of treatment is the resistance that develops due to the abandonment of the treatments.
Bacilli settle more easily in AIDS patients. The first-line treatment is usually the administration of isoniazid together with rifampicin – it’s a very effective association. It affects the areas within the caseous lesions themselves. The second line of treatment is rifampicin and pyrazinamide. They eradicate the silent or latent forms that remain in the innermost areas.
- Ethambutol: This inhibits RNA synthesis. It’s bacteriostatic, but has effective antituberculous activity. As far as adverse effects are concerned, it presents hypersensitivity and retrobulbar neurosis.
- Isoniazid: This inhibits the synthesis of mycolic acid, a lipid constituent of mycobacteria, thus killing the cell. It produces adverse hepatic and neurological reactions. To reverse it, pyridoxine is administered, because the toxic effect is due to its depletion. It’s the first choice in the treatment and prophylaxis of tuberculosis.
- Pyrazinamide: The exact mechanism of action isn’t known. It’s bactericidal against M. tuberculosis only in an acid medium. Furthermore, it’s more effective against intracellular bacilli and also in low oxygen lesions. It’s administered orally in combination with isoniazid and rifampicin. The main adverse reaction here is the high hepatotoxicity it produces.
Other antibacterials
Other commonly-used antibiotics are:
- Nitrofurantoin: in a urinary antiseptic against Gram bacteria -. They’re unstable metabolites that break bacterial DNA.
- Mupirocin: This is for topical administration. It prevents the incorporation of isoleucine into cell walls. It’s also associated with healing agents to promote healing.
- Fosfomycin: This inhibits the cell wall. It’s broad-spectrum and is used to treat the elderly with respiratory problems.
- Oxazolidinones: linezolid inhibits protein synthesis by binding to the 50S subunit of ribosomes. It’s used for patients with pneumonia, but you must be careful with heart problems.
Antibiotic resistance
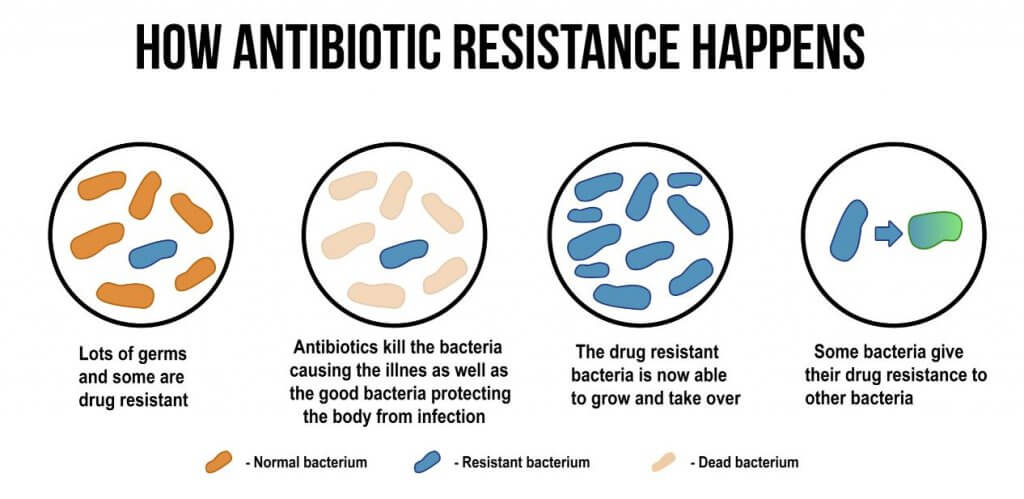
Well, when strains are resistant to antibiotics, it basically means that this antibiotic is no longer effective against that bacterium. But how can that happen? There are various mechanisms that these microorganisms develop to defend themselves against the effect of the drug.
On the other hand, you may think that if one particular drug is no longer effective against that bacteria, then we can use another and the problem ends. Yes, that is indeed one solution we have today, but the problem is that we often abuse the use of antibiotics, and the bacteria that are being treated with the other antibiotic can also become resistant to that one.
As a result, there are fewer and fewer antibiotics that we have to fight against pathogenic bacteria and we could be left without a cure. The development of new drugs is a complex, long, and very expensive process. For this reason, it’s extremely important not to self-medicate and always follow the doctor’s recommendations.
Antibiotics are chemical substances produced by a living being, or synthetic derivatives of them that kill or prevent the growth of certain classes of sensitive microorganisms. Generally, they’re drugs used in the treatment of bacterial infections. That’s why they’re known as antibacterials, and are used in human and animal medicine.
They generally help the person or animal’s defenses until local responses are able to control the infection. The objective of antibiotic treatment is to achieve the eradication of the pathogenic or bacterial microorganism.
In order to do this, it’s necessary to follow a dosage that achieves a drug concentration higher than the minimum concentration – one that’s capable of interfering with the proliferation of the microorganism involved in the infection. However, self-medication with antibiotics is a serious public health problem, and we’ll talk about it a bit later in the article.
The history of antibiotics
The first antibiotic was penicillin and was discovered in 1897 by Ernest Duchesne, in France. The scientist worked with fungi of the genus Penicillium. However, his work didn’t receive the attention of the scientific community.
Later on, Alexander Fleming, a British physician, was growing the Staphylococcus aureus bacteria on a petri dish. The culture was accidentally contaminated by fungi, and, as a result, he noticed that the growth around the mold was free of bacteria.
Although he couldn’t purify the material obtained, he published the discovery in the scientific literature. Since the fungus was of the genus Penicillium, the substance that interfered with this bacterial growth would be called penicillin.
The discovery of antibiotics, like other important discoveries such as anesthesia or the adoption of hygienic practices, revolutionized medicine and became one of the great advances in the history of medicine. Next, we’ll look at the following points about antibiotics:
- Classes of antibiotics
- Classification
- Antibiotic resistance
Classes of antibiotics
Unlike the previous ones, Gram – bacteria have a more complex cell wall. They have an inner cell wall, a peptidoglycan wall, and an outer lipid bilayer. To find out if a bacterium is Gram + or Gram – Gram staining is performed in the laboratory.
Those with a positive sign will turn blue or purple, while those with a negative sign will turn red. In this sense, narrow-spectrum antibiotics are only effective against one type of bacteria, either Gram + or Gram -.
On the contrary, broad-spectrum ones are effective against both types of bacteria. In addition to this type of antibiotic, it’s necessary to differentiate between those that are bacteriostatic and those that are bactericidal. The former are those that inhibit the growth of the microorganism without inducing its death. On the other hand, bactericides do induce the death of the bacteria. Some bacteriostatic antibiotics can be considered bactericidal above a certain concentration.
Classification
The classification of these drugs is established according to the mechanism of action they trigger. Thus, we can find the following drugs:
1. Inhibitors of cell wall synthesis
Bacteria of the Mycoplasma, Chlamydia and Rickettsia genera don’t have a cell wall, and so they’re resistant to this type of antibiotic. Within this group, we differentiate between beta-lactams, glucopectidics, and bacitracin A.
a) Beta-lactams
They’re narrow-spectrum drugs, since they’re only effective against Gram + bacteria; in addition, they’re bactericidal. These medications are administered orally and parenterally. In addition, they’re very safe drugs as the possible adverse reactions are just limited to possible allergic reactions.
They can penetrate the placenta, but, despite this, they can still be used during pregnancy. They’re used for all kinds of infections, and, among the most common, we can find:
- Penicillin
- Cephalosporins
- Monobactams (active against Gram – bacteria)
- Carbapenems
b) Glycopeptides
These antibiotics inhibit the synthesis of the cell wall from the outside, and they’re also bactericidal. Their main characteristic is that they reduce the resistance that bacteria can develop, and ensure the effectiveness of other antibiotics.
They facilitate the reduction of the peptidoglycan framework of Gram – bacteria. Because of this, they favor the action of specific drugs against these bacteria. However, glycopeptides are particularly effective against Gram + bacteria.
A typical pharmacological combination is the administration of aminoglycosides (which inhibit protein synthesis) with vancomycin, which favors the action of aminoglycosides. Vancomycin – the most representative drug in this group – is administered intravenously.
Caution must be exercised because it’s a drug with a high toxicity, and, if the infusion is too quick, then the patient may suffer from red neck syndrome. It can also be given orally, but only for the treatment of pseudomembranous colitis. If administered intravenously, the main indication is to treat infections resistant to penicillins and cephalosporins, or people allergic to the latter.
c) Bacitracin A
This drug inhibits the regeneration of peptidoglycan transporter lipid. It has a narrow spectrum, as it’s only effective against infections by Gram + bacteria. It’s administered topically, as the intramuscular route is very painful, and it presents a lot of toxicity intravenously. For this reason, it’s used in eye, skin, and throat infections.
2. Interference with membrane function
Thus, the components of the cell leave and cell lysis occurs. They’re effective against Gram – and are administered topically. They’re often associated with bacitracin A or neomycin. As for Na colistemetate, its use is limited to hospitals, and it’s primarily used in respiratory infections and cystic fibrosis.
3. Inhibitors of protein synthesis
- Aminoglycosides
- Streptogramins
- Macrolides
- Lincosamides
- Tetracyclines
- Amphenicols
a) Aminoglycosides
Gentamicin is the most widely used. These antibiotics enter the cell by active transport. Upon reaching the cytoplasm, they irreversibly bind to the 30S subunit of ribosomes. In this way, they decrease protein synthesis or cause proteins to be synthesized as defective proteins. They’re active against Gram – bacteria.
Due to their low bioavailability, its use is limited to intravenous administration in hospitals. However, it can also be administered intramuscularly in an outpatient setting. The most serious adverse reactions are ototoxicity and nephrotoxicity. This is because these structures are similar to the cell membrane, and due to the fact that aminoglycosides bind and accumulate.
As a result, continuous use at high doses can cause deafness and kidney problems. The regimen of administration of these antibiotics is by rapid infusion, and for a short period of time so that it doesn’t accumulate, thus reducing adverse reactions. Its main use is for serious infections by Enterobacteriaceae and Pseudomonas aeruginosa.
b) Streptogramins
c) Macrolides
These antibiotics bind to the 50S subunit, inhibiting translocation. They’re bacteriostatic, although there are some with bactericidal action. They’re broad-spectrum, but are more effective against Gram +. Besides, they’re also a good alternative to penicillins. Erythromycin is the best option for pertussis. They’re also effective in treating respiratory infections and non-hospital pneumonia.
d) Lincosamides
These are also similar to macrolides. They’re systemically aggressive drugs because they cause pseudomembranous colitis. For this reason, it’s limited to topical use.
c) Tetracyclines
They enter the cell by passive diffusion because they’re very fat-soluble, and they can also use active transport coupled with some alterable transporter. On the other hand, oral absorption is regular, and decreases with the intake of food (it shouldn’t be taken with milk or dairy) and with divalent cations because they can form complexes.
They’re widely distributed throughout the body and have a high affinity for developing bones and teeth, and they can turn yellow or brown, especially in children. It’s worth mentioning that the most characteristic adverse reactions of these drugs affect the digestive system. These antibiotics are contraindicated in the gestation period, during lactation, and in children under 8 years of age.
d) Amphenicols
The most powerful antibiotic in this group is chloramphenicol. Its mechanism of action is that the drug enters the cell by facilitated diffusion to bind to the 50S subunit of its ribosomes. They inhibit the binding of aminoacyl tRNA and consequently inhibit protein synthesis and therefore bacterial proliferation.
For this reason, they’re bacteriostatic. If this process occurs in eukaryotic cells of the body, then toxicity will occur, especially in the bone marrow. Developed countries avoid using it and use others that are more expensive and safer.
Its administration is reduced as an alternative in people allergic to cephalosporins in bacterial meningitis and tetracyclines in cases of Rocky Mountain fever. In developing countries, the benefit is greater than the risk, which is why it is used primarily to treat enteric fever.
4. Inhibition of DNA synthesis
We can distinguish between two groups:
Quinolones and fluoroquinolones
The former are narrow-spectrum while the fluoroquinolones are broad-spectrum. They decrease the activity of the DNA gyrase. At high concentrations, the activity of topoisomerase II, both bacterial and human, also decreases, and so it could have some antineoplastic action. They’re used in infections of all kinds, as prophylactics in immunosuppressed people and in people who have resistance to tuberculosis.
Nitroimidazole
These are antibacterial, antifungal, and antiparasitic. Its activity requires 5′-nitro reduction by enzymes called nitroreductases. Intermediates are cytotoxic, thus reducing DNA synthesis. They’re bactericidal with reduced action because the enzymes necessary for these antibiotics to take effect are not found in all bacteria. It should be mentioned that metronidazole is mutagenic.
5. Inhibitors of RNA synthesis
This group is represented by rifampicins. They’re effective against mycobacteria, Gram + bacteria, and some Gram – bacteria. They’re used in the treatment of tuberculosis, and inhibit RNA synthesis by blocking RNA polymerase. Depending on the concentration administered, they’re bactericidal or bacteriostatic antibiotics. We can highlight 3 drugs from this group:
- Rifampicin: This is the most used in tuberculosis and leprosy. Produces hepatotoxicity.
- Rifaximin: This is an intestinal anti-infective.
- Rifabutin: Prevents Mycobacterium avium-intracellulare infections and is effective in difficult-to-treat infections – especially in immunosuppressed patients.
6. Inhibition of folic acid synthesis
a) Sulfamides
Sulfadiazine is the reference drug in this group, and inhibits the DHFS enzyme. One of its adverse reactions is allergy-related, and it’s administered topically and systemically. Bacteria can develop resistance to these drugs if they decrease the permeability of the cell membrane.
b) Sulfones
The most widely-used drug in this family is dapsone and it’s effective against the bacterium Mycobacterium leprae. It is, therefore, an antileprosy drug.
7. DHPR inhibitors
Within this group we can mention:
- Trimethoprim: This is a bacteriostatic which can be given alone or with sulfa drugs. It’s the choice option for acute and chronic urinary infections. It’s also used for respiratory infections, pneumonia, and gastroenteritis.
- Pyrimethamine: This is an antiparasitic, and is used for the treatment of malaria.
- Trimetexate: It inhibits DHFR in humans. For that reason, it inhibits the proliferation of eukaryotic, neoplastic, and immune cells. Therefore, it has an antineoplastic effect similar to that of methotrexate.
8. Anti-tuberculosis and anti-leprosy
Treatment tries to quickly control and kill the bacilli that cause the disease and also prevents or decreases the number of relapses. These are very long treatments with more than one active principle. The problem with this type of treatment is the resistance that develops due to the abandonment of the treatments.
Bacilli settle more easily in AIDS patients. The first-line treatment is usually the administration of isoniazid together with rifampicin – it’s a very effective association. It affects the areas within the caseous lesions themselves. The second line of treatment is rifampicin and pyrazinamide. They eradicate the silent or latent forms that remain in the innermost areas.
- Ethambutol: This inhibits RNA synthesis. It’s bacteriostatic, but has effective antituberculous activity. As far as adverse effects are concerned, it presents hypersensitivity and retrobulbar neurosis.
- Isoniazid: This inhibits the synthesis of mycolic acid, a lipid constituent of mycobacteria, thus killing the cell. It produces adverse hepatic and neurological reactions. To reverse it, pyridoxine is administered, because the toxic effect is due to its depletion. It’s the first choice in the treatment and prophylaxis of tuberculosis.
- Pyrazinamide: The exact mechanism of action isn’t known. It’s bactericidal against M. tuberculosis only in an acid medium. Furthermore, it’s more effective against intracellular bacilli and also in low oxygen lesions. It’s administered orally in combination with isoniazid and rifampicin. The main adverse reaction here is the high hepatotoxicity it produces.
Other antibacterials
Other commonly-used antibiotics are:
- Nitrofurantoin: in a urinary antiseptic against Gram bacteria -. They’re unstable metabolites that break bacterial DNA.
- Mupirocin: This is for topical administration. It prevents the incorporation of isoleucine into cell walls. It’s also associated with healing agents to promote healing.
- Fosfomycin: This inhibits the cell wall. It’s broad-spectrum and is used to treat the elderly with respiratory problems.
- Oxazolidinones: linezolid inhibits protein synthesis by binding to the 50S subunit of ribosomes. It’s used for patients with pneumonia, but you must be careful with heart problems.
Antibiotic resistance
Well, when strains are resistant to antibiotics, it basically means that this antibiotic is no longer effective against that bacterium. But how can that happen? There are various mechanisms that these microorganisms develop to defend themselves against the effect of the drug.
On the other hand, you may think that if one particular drug is no longer effective against that bacteria, then we can use another and the problem ends. Yes, that is indeed one solution we have today, but the problem is that we often abuse the use of antibiotics, and the bacteria that are being treated with the other antibiotic can also become resistant to that one.
As a result, there are fewer and fewer antibiotics that we have to fight against pathogenic bacteria and we could be left without a cure. The development of new drugs is a complex, long, and very expensive process. For this reason, it’s extremely important not to self-medicate and always follow the doctor’s recommendations.
Este texto se ofrece únicamente con propósitos informativos y no reemplaza la consulta con un profesional. Ante dudas, consulta a tu especialista.







