Vertigo: Symptoms, Causes and Treatment

Vertigo is described as a feeling of dizziness with non-existent movements, which often leads to instability, nausea, and frequent vomiting. This can occur sporadically or happen frequently.
There are many different causes that, depending on where the problem originates, can be classified into central and peripheral. Once the problem has been identified, the doctor can then prescribe the corresponding treatment.
These measures include drugs, which are very varied and tend to have other more frequent clinical uses. If you’re interested in knowing a little more about this striking condition, we have prepared the following article for you.
What is vertigo?
It doesn’t have a single definition because it’s an abstract term that actually combines several different sensations. In general terms, it’s a symptom characterized by a feeling of dizziness and instability accompanied by a false sensation of movement.
It isn’t considered to be an illness, but, rather, the result of an underlying condition or conditions. This implies the existence of multiple causes, which, for practical purposes, can be divided into central and peripheral. You’ll find a review of this classification below.
To understand vertigo a little more, it’s important to consider the anatomical structures related to the feeling of stability. The basis of the problem appears to be in the nervous system, which incorporates brain structures and some nerves that transmit information through electrical impulses.
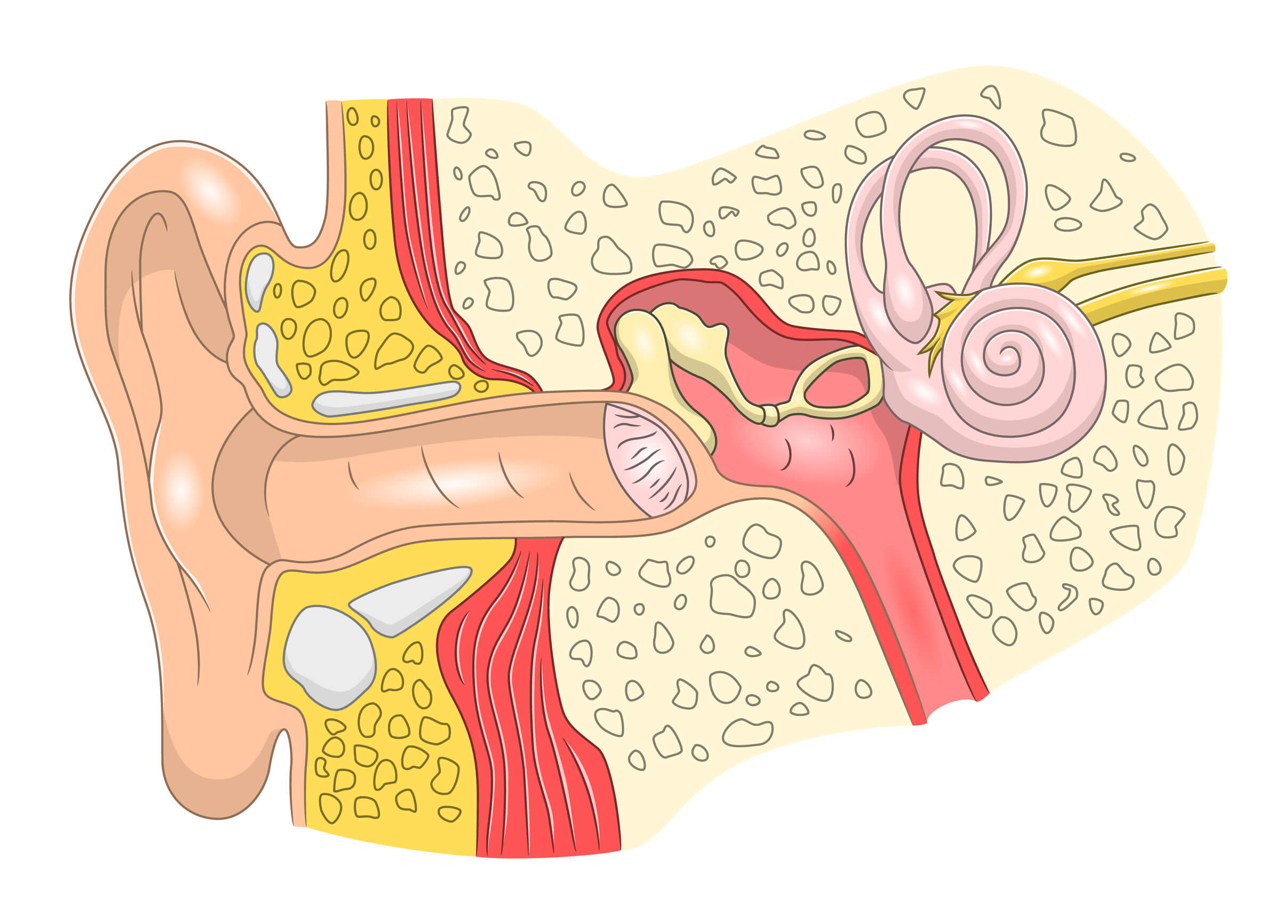
In turn, within the inner ear, there are tiny but complex structures that participate in this process. They’re responsible for collecting information thanks to the movement of small particles inside, which are affected by rotational and linear movements.
The structures within the ear are called the vestibular apparatus, and it’s made up of the semicircular, utricle, and saccule canals. They communicate in different ways and provide the information captured by the vestibulocochlear nerve, also known as the eighth cranial nerve. This is then directed to specialized brain centers.

How common is this condition?
Vertigo is usually a common cause of emergency department visits, especially when the onset is abrupt and is accompanied by other symptoms. According to a recent review article (2019), it could be the third most common symptom treated in hospitals.
So much so, that according to epidemiological data from the United States of America, acute vestibular syndrome associated with vertigo could represent up to 800,000 annual visits to the emergency room.
In Spain, research has shown just what an impact vertigo has on public health. For example, this study, carried out in 2009 in the autonomous region of Valencia, showed a prevalence of 17.8 patients per 100,000 inhabitants in the year of study.
They also concluded that the most common age to suffer it was between 50 and 60 years of age, in addition to the fact that around half of the consultations were for symptoms experienced for the first time.
Main clinical manifestations
In general, patients report instability when they keep their eyes open. There’s usually a sensation of movement despite the person being still, causing involuntary loss of balance and frequent falls.
In some cases, it can be triggered by situations such as stress, which also has other negative health effects.
In most cases, patients need to keep their eyes closed in order to feel at ease, preferring rest positions to avoid the appearance of dizziness. Nausea and vomiting are common, and they tend to decrease the quality of life when they persist.
Depending on the cause, vertigo could be associated with other symptoms. These causes can be central or peripheral, depending on the part of the body that’s affected. In the first case, they’re the organs of the central nervous system, while in the second there’s a lesion of the vestibular apparatus (in the inner ear).
Some of the associated symptoms, depending on the cause, are the following:
- Central origin: Headache, abnormal movements, and severe instability. Symptoms usually appear progressively and the duration is constant.
- Peripheral origin: Nausea, vomiting, and profuse sweating predominate. They’re usually aggravated by movements and appear intermittently or paroxysmally.
Causes of vertigo
Some of the most common causes will be summarized below based on the origin of the problem.
Peripherals
In this case, we’ll consider four common diseases.
- Benign Paroxysmal Positional Vertigo: This is usually benign and is the most common cause of vertigo. It’s characterized by episodes of less than a minute in duration, triggered by certain positions. It doesn’t usually require treatment, and may become more frequent during episodes of otitis media, trauma, or advancing age.
- Vestibular neuritis: This is the inflammation of the vestibular nerve. It usually appears abruptly, is unilateral and rarely has associated symptoms, such as tinnitus. It’s thought to occur due to the reactivation of a herpes virus (HSV-1) acquired during a previous infection, and it usually occurs in the coldest months of the year.
- Ménière’s disease: This is produced by the accumulation of fluid inside the inner ear, known as endolymph. It generates acute vertigo attacks, associated with a temporary decrease in hearing capacity and tinnitus (the perception of a high-pitched beep or sound).
- Perilymphatic fistula: This is an anatomical defect that usually occurs after some interventions, such as stapedectomy, or in the context of localized trauma. Treatment is surgical and in most cases recovery is successful.
Centrals
Unlike the previous section, vertigo of central origin doesn’t have so many associated causes. It’s usually due to two well-differentiated syndromes: vestibular migraine and vertebrobasilar infarction. Both share a vascular origin.
Vestibular migraine is characterized by severe headaches, which don’t go away even after the administration of commonly used analgesics (such as paracetamol ). It can last for several hours without showing any significant improvement, and is thought to be due to vasodilation and constriction of cerebral vessels.
Like other forms of migraine, it’s characterized by having several associated symptoms. In this specific case, vertigo is the most striking and can be even more limiting than the headaches. It can occur both with the performance of cephalic movements (rotational) and at rest.
Patients may report auditory symptoms such as tinnitus, decreased hearing, and intolerance to loud sounds, in part due to the pain that this produces.
On the other hand, vertebrobasilar infarction is included within cerebrovascular diseases. It’s due to the obstruction of a branch that supplies the vestibular system, which causes any of the aforementioned symptoms.
The difference here is the evident deterioration of motor and sensory capacity, which, depending on the affected branch, may or may not be evident. Unlike many of the aforementioned diseases, this one can be fatal, greatly affecting older people. Atherosclerosis is usually involved in its appearance.
Diagnosis
Despite the fact that there are complementary tests, most of the aforementioned conditions have a clinical diagnosis. To do this, the doctor will resort to a personal interview and a neurological physical examination, in order to determine the anatomical origin of the lesion that causes the symptoms.
Depending on the clinical manifestations, the doctor may request the following studies:
- Audiometry: This allows the doctor to measure hearing quality in patients who also have occasional vertigo.
- Tympanometry: Similar to the previous one, although it looks for anatomical and functional alterations in the middle ear and eardrum.
- Electronystagmography: Thanks to the evaluation of eye movements known as nystagmus, it’s possible to determine the cause of some syndromes that include vertigo and dizziness.
- Computed tomography: This allows the doctors to visualize areas of infarction in the first moments of a vertebrobasilar infarction, something very useful for other cerebrovascular diseases.
- Nuclear magnetic resonance: This is an imaging technique that doesn’t emit radiation and is used to assess nerve structures in detail.
Vertigo treatment
There are pharmacological and non-pharmacological therapeutic options. This depends on the cause of the symptoms, which is why self-medication usually isn’t effective. The medications, which we’ll refer to in this section, seek to temporarily reduce vertigo.
In order to do this, doctors will use drugs that intervene in the nerve pathways of transmission of stimuli related to balance. There are others that have the ability to interact with brain receptors and modulate the activity of certain neurotransmitters. They are mostly used for other purposes, but they’re also effective in treating vertigo.
- Antihistamines, as their name suggests, block the effects of histamine. They’re generally used to reduce allergic symptoms, and can induce sleep as an adverse effect, especially the first generation, which are older.
- Anticholinergics, which work in a similar way to the previous group, but seek to block the effects of acetylcholine.
- Antidopaminergics, which serve to block the function of dopamine. They serve to eliminate the feeling of nausea and vomiting. Fortunately, many of these drugs also have an antihistamine effect. An example is thiethylperazine.
- In some cases where a possible vascular cause is suspected, the administration of vasodilators may be helpful. These drugs promote increased blood flow to the structures of the vestibular apparatus. Betahistine is a representative example.
Which doctor to go to?
There are several specialists capable of diagnosing the origin of vertigo. It’s possible that in the emergency services, the first contact will be with a general practitioner or internist. In specific cases, they could refer another professional for follow-up and more specific studies.
Neurologists, otolaryngologists, and geriatricians are some of the specialists who specialize in treating different causes of vertigo.
Vertigo must be diagnosed and treated early
Vertigo is a symptom that could be the expression of an underlying disease. Although it’s rarely fatal, it tends to greatly decrease a person’s quality of life. Knowing the main causes and going to the doctor as soon as possible could help to solve the problem faster.
Vertigo is described as a feeling of dizziness with non-existent movements, which often leads to instability, nausea, and frequent vomiting. This can occur sporadically or happen frequently.
There are many different causes that, depending on where the problem originates, can be classified into central and peripheral. Once the problem has been identified, the doctor can then prescribe the corresponding treatment.
These measures include drugs, which are very varied and tend to have other more frequent clinical uses. If you’re interested in knowing a little more about this striking condition, we have prepared the following article for you.
What is vertigo?
It doesn’t have a single definition because it’s an abstract term that actually combines several different sensations. In general terms, it’s a symptom characterized by a feeling of dizziness and instability accompanied by a false sensation of movement.
It isn’t considered to be an illness, but, rather, the result of an underlying condition or conditions. This implies the existence of multiple causes, which, for practical purposes, can be divided into central and peripheral. You’ll find a review of this classification below.
To understand vertigo a little more, it’s important to consider the anatomical structures related to the feeling of stability. The basis of the problem appears to be in the nervous system, which incorporates brain structures and some nerves that transmit information through electrical impulses.
In turn, within the inner ear, there are tiny but complex structures that participate in this process. They’re responsible for collecting information thanks to the movement of small particles inside, which are affected by rotational and linear movements.
The structures within the ear are called the vestibular apparatus, and it’s made up of the semicircular, utricle, and saccule canals. They communicate in different ways and provide the information captured by the vestibulocochlear nerve, also known as the eighth cranial nerve. This is then directed to specialized brain centers.
How common is this condition?
Vertigo is usually a common cause of emergency department visits, especially when the onset is abrupt and is accompanied by other symptoms. According to a recent review article (2019), it could be the third most common symptom treated in hospitals.
So much so, that according to epidemiological data from the United States of America, acute vestibular syndrome associated with vertigo could represent up to 800,000 annual visits to the emergency room.
In Spain, research has shown just what an impact vertigo has on public health. For example, this study, carried out in 2009 in the autonomous region of Valencia, showed a prevalence of 17.8 patients per 100,000 inhabitants in the year of study.
They also concluded that the most common age to suffer it was between 50 and 60 years of age, in addition to the fact that around half of the consultations were for symptoms experienced for the first time.
Main clinical manifestations
In general, patients report instability when they keep their eyes open. There’s usually a sensation of movement despite the person being still, causing involuntary loss of balance and frequent falls.
In some cases, it can be triggered by situations such as stress, which also has other negative health effects.
In most cases, patients need to keep their eyes closed in order to feel at ease, preferring rest positions to avoid the appearance of dizziness. Nausea and vomiting are common, and they tend to decrease the quality of life when they persist.
Depending on the cause, vertigo could be associated with other symptoms. These causes can be central or peripheral, depending on the part of the body that’s affected. In the first case, they’re the organs of the central nervous system, while in the second there’s a lesion of the vestibular apparatus (in the inner ear).
Some of the associated symptoms, depending on the cause, are the following:
- Central origin: Headache, abnormal movements, and severe instability. Symptoms usually appear progressively and the duration is constant.
- Peripheral origin: Nausea, vomiting, and profuse sweating predominate. They’re usually aggravated by movements and appear intermittently or paroxysmally.
Causes of vertigo
Some of the most common causes will be summarized below based on the origin of the problem.
Peripherals
In this case, we’ll consider four common diseases.
- Benign Paroxysmal Positional Vertigo: This is usually benign and is the most common cause of vertigo. It’s characterized by episodes of less than a minute in duration, triggered by certain positions. It doesn’t usually require treatment, and may become more frequent during episodes of otitis media, trauma, or advancing age.
- Vestibular neuritis: This is the inflammation of the vestibular nerve. It usually appears abruptly, is unilateral and rarely has associated symptoms, such as tinnitus. It’s thought to occur due to the reactivation of a herpes virus (HSV-1) acquired during a previous infection, and it usually occurs in the coldest months of the year.
- Ménière’s disease: This is produced by the accumulation of fluid inside the inner ear, known as endolymph. It generates acute vertigo attacks, associated with a temporary decrease in hearing capacity and tinnitus (the perception of a high-pitched beep or sound).
- Perilymphatic fistula: This is an anatomical defect that usually occurs after some interventions, such as stapedectomy, or in the context of localized trauma. Treatment is surgical and in most cases recovery is successful.
Centrals
Unlike the previous section, vertigo of central origin doesn’t have so many associated causes. It’s usually due to two well-differentiated syndromes: vestibular migraine and vertebrobasilar infarction. Both share a vascular origin.
Vestibular migraine is characterized by severe headaches, which don’t go away even after the administration of commonly used analgesics (such as paracetamol ). It can last for several hours without showing any significant improvement, and is thought to be due to vasodilation and constriction of cerebral vessels.
Like other forms of migraine, it’s characterized by having several associated symptoms. In this specific case, vertigo is the most striking and can be even more limiting than the headaches. It can occur both with the performance of cephalic movements (rotational) and at rest.
Patients may report auditory symptoms such as tinnitus, decreased hearing, and intolerance to loud sounds, in part due to the pain that this produces.
On the other hand, vertebrobasilar infarction is included within cerebrovascular diseases. It’s due to the obstruction of a branch that supplies the vestibular system, which causes any of the aforementioned symptoms.
The difference here is the evident deterioration of motor and sensory capacity, which, depending on the affected branch, may or may not be evident. Unlike many of the aforementioned diseases, this one can be fatal, greatly affecting older people. Atherosclerosis is usually involved in its appearance.
Diagnosis
Despite the fact that there are complementary tests, most of the aforementioned conditions have a clinical diagnosis. To do this, the doctor will resort to a personal interview and a neurological physical examination, in order to determine the anatomical origin of the lesion that causes the symptoms.
Depending on the clinical manifestations, the doctor may request the following studies:
- Audiometry: This allows the doctor to measure hearing quality in patients who also have occasional vertigo.
- Tympanometry: Similar to the previous one, although it looks for anatomical and functional alterations in the middle ear and eardrum.
- Electronystagmography: Thanks to the evaluation of eye movements known as nystagmus, it’s possible to determine the cause of some syndromes that include vertigo and dizziness.
- Computed tomography: This allows the doctors to visualize areas of infarction in the first moments of a vertebrobasilar infarction, something very useful for other cerebrovascular diseases.
- Nuclear magnetic resonance: This is an imaging technique that doesn’t emit radiation and is used to assess nerve structures in detail.
Vertigo treatment
There are pharmacological and non-pharmacological therapeutic options. This depends on the cause of the symptoms, which is why self-medication usually isn’t effective. The medications, which we’ll refer to in this section, seek to temporarily reduce vertigo.
In order to do this, doctors will use drugs that intervene in the nerve pathways of transmission of stimuli related to balance. There are others that have the ability to interact with brain receptors and modulate the activity of certain neurotransmitters. They are mostly used for other purposes, but they’re also effective in treating vertigo.
- Antihistamines, as their name suggests, block the effects of histamine. They’re generally used to reduce allergic symptoms, and can induce sleep as an adverse effect, especially the first generation, which are older.
- Anticholinergics, which work in a similar way to the previous group, but seek to block the effects of acetylcholine.
- Antidopaminergics, which serve to block the function of dopamine. They serve to eliminate the feeling of nausea and vomiting. Fortunately, many of these drugs also have an antihistamine effect. An example is thiethylperazine.
- In some cases where a possible vascular cause is suspected, the administration of vasodilators may be helpful. These drugs promote increased blood flow to the structures of the vestibular apparatus. Betahistine is a representative example.
Which doctor to go to?
There are several specialists capable of diagnosing the origin of vertigo. It’s possible that in the emergency services, the first contact will be with a general practitioner or internist. In specific cases, they could refer another professional for follow-up and more specific studies.
Neurologists, otolaryngologists, and geriatricians are some of the specialists who specialize in treating different causes of vertigo.
Vertigo must be diagnosed and treated early
Vertigo is a symptom that could be the expression of an underlying disease. Although it’s rarely fatal, it tends to greatly decrease a person’s quality of life. Knowing the main causes and going to the doctor as soon as possible could help to solve the problem faster.
- Alcalá T, Lambert M, Suárez A. Enfoque clínico del vértigo desde la Atención Primaria
de Salud. Revista Habanera de Ciencias Médicas 2014;13(3):394-405. - Harari N, Roa F. Vértigo: revisión de los principales trastornos periféricos y centrales. An Med (Mex) 2019;64(4):290-296.
- Lopez-Escamez J, et al. Criterios diagnósticos de enfermedad de Menière. Documento de consenso de la Bárány Society, la Japan Society for Equilibrium Research, la European Academy of Otology and Neurotology (EAONO), la American Academy of Otolaryngology-Head and Neck Surgery (AAO-HNS) y la Korean Balance Society. Acta Otorrinolaringológica Española 2016;67(1):1-7.
- Martín-Aragón S, Bermejo-Bescós P. Vértigo. Tratamiento farmacológico. Of 2010;29(1):74-78.
- Romero F. Neuronitis vestibular. Faso 2015;22(1):61-64.
- Saber A, et al. Small strokes causing severe vertigo. Frequency of false-negative MRIs and nonlacunar mechanisms. Neurology 2014;83:169-173.
Este texto se ofrece únicamente con propósitos informativos y no reemplaza la consulta con un profesional. Ante dudas, consulta a tu especialista.







